

Health related quality of life in multimorbidity: a primary-care based study from Odisha, India
- PMID: 31277648
- PMCID: PMC6612103
- DOI: 10.1186/s12955-019-1180-3
Health related quality of life in multimorbidity: a primary-care based study from Odisha, India
Abstract
Background: Multimorbidity, the coexistence of two or more chronic conditions is increasingly prevalent in primary care populations. Despite reports on its adverse impact on health outcomes, functioning and well-being, it's association with quality of life is not well known in low and middle income countries. We assessed the health-related quality of life (HRQoL) of primary care patients with multimorbidity and identified the influencing factors.
Methods: This cross-sectional study was done across 20 public and 20 private primary care facilities in Odisha, India. Data were collected from 1649 adult out-patients using a structured multimorbidity assessment questionnaire for primary care (MAQ-PC). HRQoL was assessed by the 12-item short-form health survey (SF-12). Both physical (PCS) and mental components scores (MCS) were calculated. Multiple regression analysis was performed to determine the association of HRQoL with socio-demographics, number, severity and typology of chronic conditions.
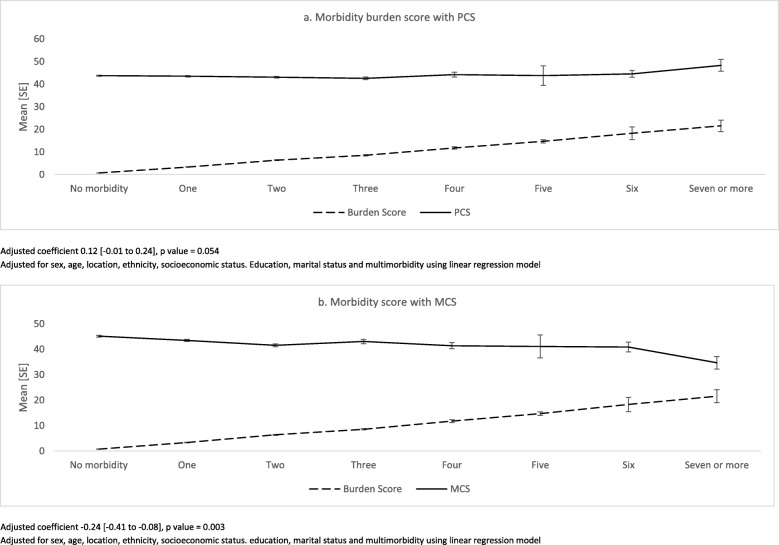
Results: Around 28.3% [95% CI: 25.9-30.7] of patients had multimorbidity. Mean physical component scope (PCS) and mental component score (MCS) of QoL in the study population was 43.56 [95% CI: 43.26-43.86] and 43.69 [95% CI: 43.22-44.16], respectively. Patients with multimorbidity reported poorer mean PCS [43.23, 95% CI: 42.62-43.84] and MCS [41.58, 95% CI: 40.74-42.43] compared to those without. After adjusting for other variables, morbidity severity burden score was found to be negatively associated with MCS [adjusted coefficient: -0.24, 95% CI - 0.41 to - 0.08], whereas no significant association was seen with PCS. Hypertension and diabetes with arthritis and acid peptic diseases were found to be negatively related with MCS. Within multimorbidity, lower education was inversely associated with mental QoL and positively associated with physical QoL score after adjusting for other variables.
Conclusion: Our findings demonstrate the diverse negative effects of multimorbidity on HRQoL and reveal that apart from count of chronic conditions, severity and pattern also influence HRQoL negatively. Health care providers should consider severity as an outcome measure to improve QoL especially in individuals with physical multimorbidity. Given the differences observed between age groups, it is important to identify specific care needs for each group. Musculoskeletal clusters need prioritised attention while designing clinical guidelines for multimorbidity.
Keywords: HRQoL; India; Multimorbidity; Multiple chronic conditions; Primary care; Quality of life.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Magnitude and determinants of multimorbidity and health care utilization among patients attending public versus private primary care: a cross-sectional study from Odisha, India.Int J Equity Health. 2020 Apr 29;19(1):57. doi: 10.1186/s12939-020-01170-y. Int J Equity Health. 2020. PMID: 32349770 Free PMC article.
-
Pattern and severity of multimorbidity among patients attending primary care settings in Odisha, India.PLoS One. 2017 Sep 14;12(9):e0183966. doi: 10.1371/journal.pone.0183966. eCollection 2017. PLoS One. 2017. PMID: 28910309 Free PMC article. Clinical Trial.
-
Multimorbidity and quality of life: a closer look.Health Qual Life Outcomes. 2007 Aug 6;5:52. doi: 10.1186/1477-7525-5-52. Health Qual Life Outcomes. 2007. PMID: 17683600 Free PMC article.
-
Multimorbidity and quality of life in primary care: a systematic review.Health Qual Life Outcomes. 2004 Sep 20;2:51. doi: 10.1186/1477-7525-2-51. Health Qual Life Outcomes. 2004. PMID: 15380021 Free PMC article. Review.
-
The impact of rheumatoid arthritis on quality-of-life assessed using the SF-36: a systematic review and meta-analysis.Semin Arthritis Rheum. 2014 Oct;44(2):123-30. doi: 10.1016/j.semarthrit.2014.05.001. Epub 2014 May 29. Semin Arthritis Rheum. 2014. PMID: 24973898 Review.
Cited by
-
Multimorbidity Patterns and Their Association with Social Determinants, Mental and Physical Health during the COVID-19 Pandemic.Int J Environ Res Public Health. 2022 Dec 15;19(24):16839. doi: 10.3390/ijerph192416839. Int J Environ Res Public Health. 2022. PMID: 36554719 Free PMC article.
-
Metabolomics of Multimorbidity: Could It Be the Quo Vadis?Front Mol Biosci. 2022 Mar 11;9:848971. doi: 10.3389/fmolb.2022.848971. eCollection 2022. Front Mol Biosci. 2022. PMID: 35359598 Free PMC article.
-
Systematic review on the instruments used for measuring the association of the level of multimorbidity and clinically important outcomes.BMJ Open. 2021 May 5;11(5):e041219. doi: 10.1136/bmjopen-2020-041219. BMJ Open. 2021. PMID: 33952533 Free PMC article.
-
The association between lower urinary tract symptoms secondary to benign prostatic hyperplasia and multimorbidity among Chinese middle-aged and elderly males: evidence based on propensity score matching.Transl Androl Urol. 2024 Sep 30;13(9):1932-1945. doi: 10.21037/tau-24-268. Epub 2024 Sep 26. Transl Androl Urol. 2024. PMID: 39434733 Free PMC article.
-
Exploring the non-communicable disease (NCD) network of multi-morbid individuals in India: A network analysis.PLOS Glob Public Health. 2022 Jun 30;2(6):e0000512. doi: 10.1371/journal.pgph.0000512. eCollection 2022. PLOS Glob Public Health. 2022. PMID: 36962702 Free PMC article.
References
-
- NCD Alliance Report 2012-2013. Putting non-communicable diseases on the global agenda [Internet]. WHO; 2012 [cited 2013 May 30]. Available from: www.ncdalliance.org/Report2012.
-
- van den AM, Buntinx F, Knottnerus JA. Comorbidity or multimorbidity. Eur J Gen Pract. 1996;2(2):65–70. doi: 10.3109/13814789609162146. - DOI
-
- Arokiasamy P, Uttamacharya, Jain K. Multi-Morbidity, Functional limitations, and self-rated health among older adults in India. SAGE Open 2015 [cited 2015 Apr 23];5(1). Available from: http://sgo.sagepub.com/content/5/1/2158244015571640
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
