

Characteristics of community-acquired respiratory viruses infections except seasonal influenza in transplant recipients and non-transplant critically ill patients
- PMID: 31262511
- PMCID: PMC7102620
- DOI: 10.1016/j.jmii.2019.05.007
Characteristics of community-acquired respiratory viruses infections except seasonal influenza in transplant recipients and non-transplant critically ill patients
Abstract
Background/purpose: Transplant recipients are vulnerable to life-threatening community-acquired respiratory viruses (CA-RVs) infection (CA-RVI). Even if non-transplant critically ill patients in intensive care unit (ICU) have serious CA-RVI, comparison between these groups remains unclear. We aimed to evaluate clinical characteristics and mortality of CA-RVI except seasonal influenza A/B in transplant recipients and non-transplant critically ill patients in ICU.
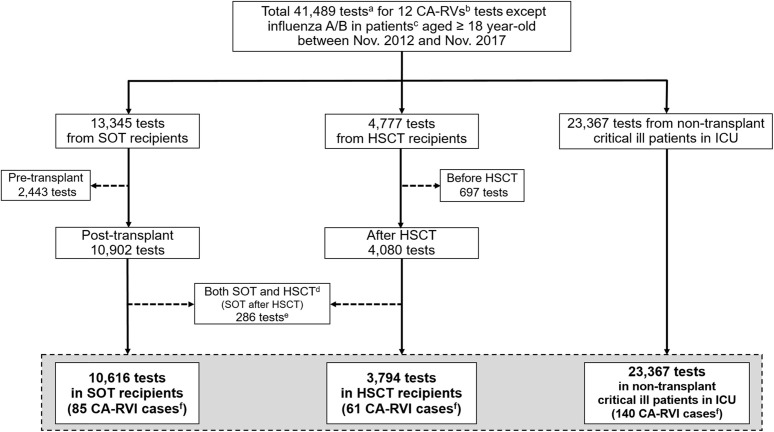
Methods: We collected 37,777 CA-RVs multiplex real-time reverse transcription-polymerase chain reaction test results of individuals aged ≥18 years from November 2012 to November 2017. The CA-RVs tests included adenovirus, coronavirus 229E/NL63/OC43, human bocavirus, human metapneumovirus, parainfluenza virus 1/2/3, rhinovirus, and respiratory syncytial virus A/B.
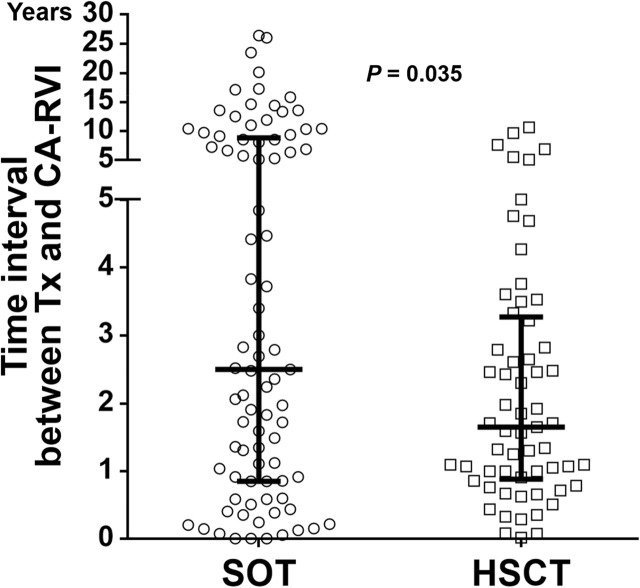
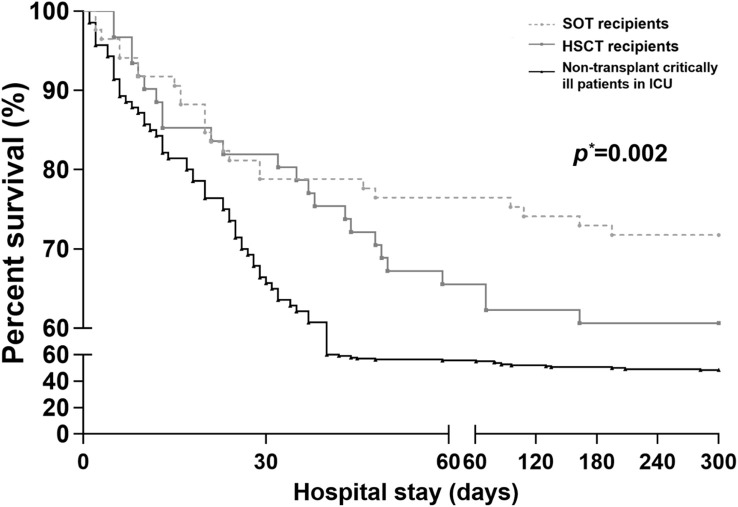
Results: We found 286 CA-RVI cases, including 85 solid organ transplantation recipients (G1), 61 hematopoietic stem cell transplantation recipients (G2), and 140 non-transplant critically ill patients in ICU (G3), excluding those with repeated isolation within 30 days. Adenovirus positive rate and infection cases were most prominent in G2 (p < 0.001). The median time interval between transplantation and CA-RVI was 30 and 20 months in G1 and G2, respectively. All-cause in-hospital mortality was significantly higher in G3 than in G1 or G2 (51.4% vs. 28.2% or 39.3%, p = 0.002, respectively). The mechanical ventilation (MV) was the independent risk factor associated with all-cause in-hospital mortality in all three groups (hazard ratio, 3.37, 95% confidence interval, 2.04-5.56, p < 0.001).
Conclusions: This study highlights the importance of CA-RVs diagnosis in transplant recipients even in long-term posttransplant period, and in non-transplant critically ill patients in ICU with MV.
Keywords: Community-acquired respiratory viruses; Critically ill patients; Hematopoietic stem cell transplantation; Mortality; Solid organ transplantation.
Copyright © 2019. Published by Elsevier B.V.
Figures
Similar articles
-
A Multicenter Consortium to Define the Epidemiology and Outcomes of Pediatric Solid Organ Transplant Recipients With Inpatient Respiratory Virus Infection.J Pediatric Infect Dis Soc. 2019 Jul 1;8(3):197-204. doi: 10.1093/jpids/piy024. J Pediatric Infect Dis Soc. 2019. PMID: 29538674 Free PMC article.
-
Seasonal Human Coronavirus Respiratory Tract Infection in Recipients of Allogeneic Hematopoietic Stem Cell Transplantation.J Infect Dis. 2021 May 20;223(9):1564-1575. doi: 10.1093/infdis/jiaa553. J Infect Dis. 2021. PMID: 32860509 Free PMC article.
-
Clinical Significance of Upper Airway Virus Detection in Critically Ill Hematology Patients.Am J Respir Crit Care Med. 2019 Feb 15;199(4):518-528. doi: 10.1164/rccm.201804-0681OC. Am J Respir Crit Care Med. 2019. PMID: 30230909
-
Community respiratory virus infections in immunocompromised patients: hematopoietic stem cell and solid organ transplant recipients, and individuals with human immunodeficiency virus infection.Semin Respir Crit Care Med. 2007 Apr;28(2):222-42. doi: 10.1055/s-2007-976494. Semin Respir Crit Care Med. 2007. PMID: 17458776 Review.
-
Community respiratory viruses: organ transplant recipients.Am J Med. 1997 Mar 17;102(3A):31-6; discussion 42-3. doi: 10.1016/s0002-9343(97)80008-3. Am J Med. 1997. PMID: 10868140 Review.
Cited by
-
Emerging threats from zoonotic coronaviruses-from SARS and MERS to 2019-nCoV.J Microbiol Immunol Infect. 2020 Jun;53(3):365-367. doi: 10.1016/j.jmii.2020.02.001. Epub 2020 Feb 4. J Microbiol Immunol Infect. 2020. PMID: 32035811 Free PMC article. No abstract available.
-
Human gene polymorphisms and their possible impact on the clinical outcome of SARS-CoV-2 infection.Arch Virol. 2021 Aug;166(8):2089-2108. doi: 10.1007/s00705-021-05070-6. Epub 2021 May 2. Arch Virol. 2021. PMID: 33934196 Free PMC article. Review.
-
Treatment options for COVID-19: The reality and challenges.J Microbiol Immunol Infect. 2020 Jun;53(3):436-443. doi: 10.1016/j.jmii.2020.03.034. Epub 2020 Apr 4. J Microbiol Immunol Infect. 2020. PMID: 32307245 Free PMC article. Review.
-
Knowledge toward COVID-19 in children among undergraduate students at the beginning of COVID-19 era.Nurs Open. 2023 Jun;10(6):3579-3585. doi: 10.1002/nop2.1600. Epub 2023 Jan 10. Nurs Open. 2023. PMID: 36625197 Free PMC article.
-
Potential Drugs in COVID-19 Management.Curr Med Chem. 2024;31(22):3245-3264. doi: 10.2174/0929867331666230717154101. Curr Med Chem. 2024. PMID: 37461346 Review.
References
-
- Fishman J.A. Infection in solid-organ transplant recipients. N Engl J Med. 2007;357:2601–2614. - PubMed
-
- Fishman J.A., Issa N.C. Infection in organ transplantation: risk factors and evolving patterns of infection. Infect Dis Clin N Am. 2010;24:273–283. - PubMed
-
- Wingard J.R., Hsu J., Hiemenz J.W. Hematopoietic stem cell transplantation: an overview of infection risks and epidemiology. Infect Dis Clin N Am. 2010;24:257–272. - PubMed
-
- Abbas S., Raybould J.E., Sastry S., de la Cruz O. Respiratory viruses in transplant recipients: more than just a cold. Clinical syndromes and infection prevention principles. Int J Infect Dis. 2017;62:86–93. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
