

Adrenal βarrestin1 targeting for tobacco-associated cardiac dysfunction treatment: Aldosterone production as the mechanistic link
- PMID: 31236278
- PMCID: PMC6581946
- DOI: 10.1002/prp2.497
Adrenal βarrestin1 targeting for tobacco-associated cardiac dysfunction treatment: Aldosterone production as the mechanistic link
Abstract
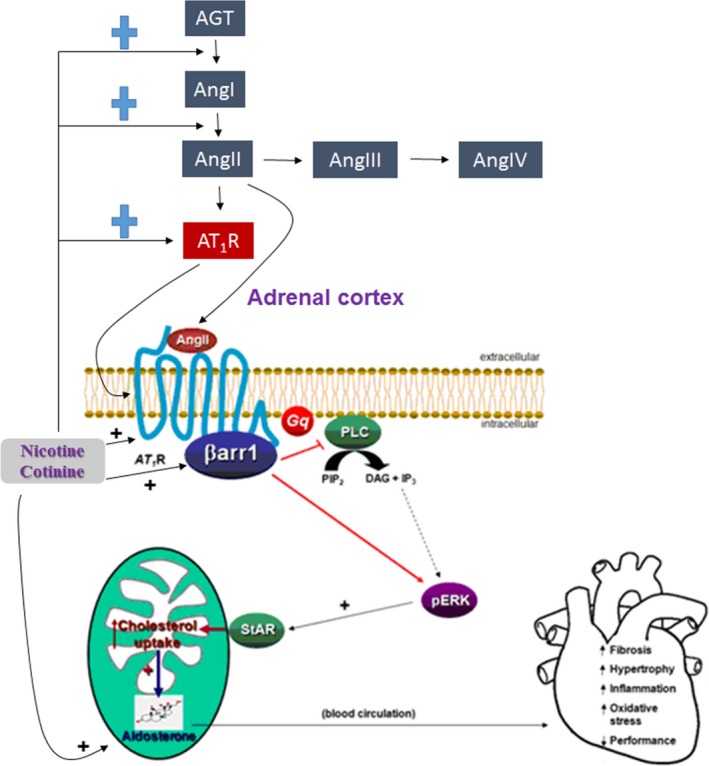
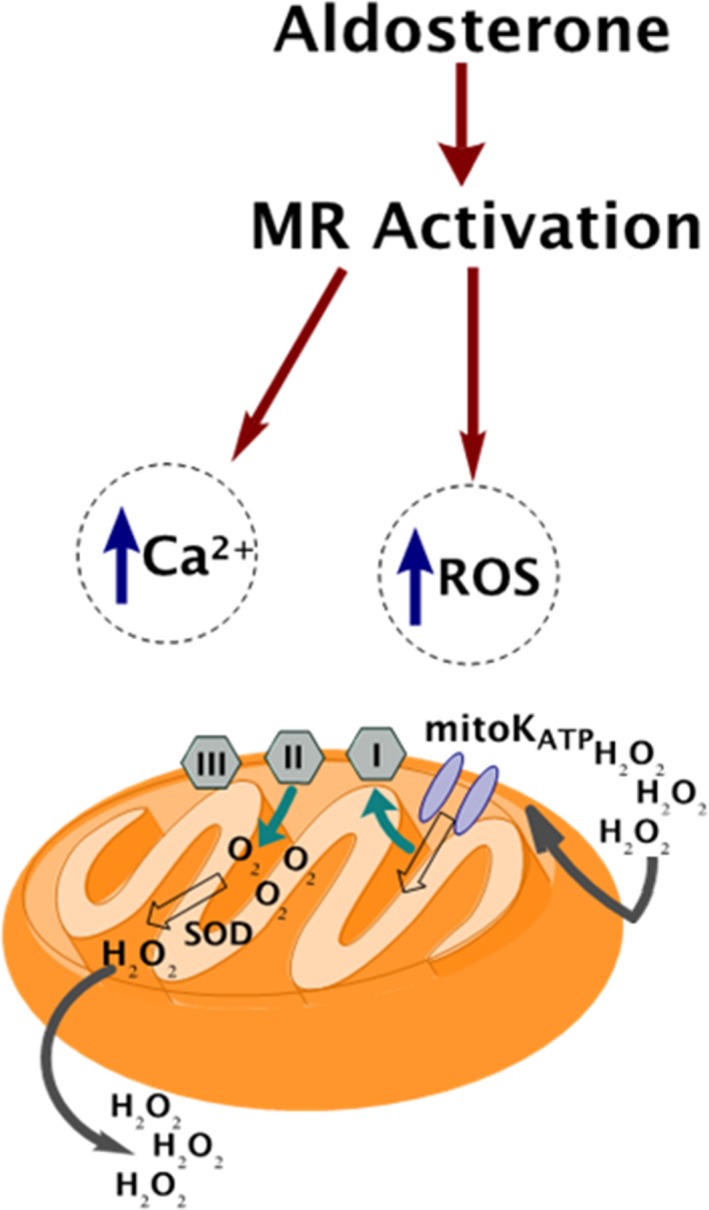
Tobacco kills 6 million people annually and its global health costs are continuously rising. The main addictive component of every tobacco product is nicotine. Among the mechanisms by which nicotine, and its major metabolite, cotinine, contribute to heart disease is the renin-angiotensin-aldosterone system (RAAS) activation. This increases aldosterone production from the adrenals and circulating aldosterone levels. Aldosterone is a mineralocorticoid hormone with various direct harmful effects on the myocardium, including increased reactive oxygen species (ROS) generation, which contributes significantly to cardiac mitochondrial dysfunction and cardiac aging. Aldosterone is produced in the adrenocortical zona glomerulosa (AZG) cells in response to angiotensin II (AngII), activating its type 1 receptor (AT1R). The AT1R is a G protein-coupled receptor (GPCR) that leads to aldosterone biosynthesis and secretion, via signaling from both Gq/11 proteins and the GPCR adapter protein βarrestin1, in AZG cells. Adrenal βarrestin1 is essential for AngII-dependent adrenal aldosterone production, which aggravates heart disease. Since adrenal βarrestin1 is essential for raising circulating aldosterone in the body and tobacco compounds are also known to elevate aldosterone levels in smokers, accelerating heart disease progression, our central hypothesis is that nicotine and cotinine increase aldosterone levels to induce cardiac injury by stimulating adrenal βarrestin1. In the present review, we provide an overview of the current literature of the physiology and pharmacology of adrenal aldosterone production regulation, of the effects of tobacco on this process and, finally, of the effects of tobacco and aldosterone on cardiac structure and function, with a particular focus on cardiac mitochondrial function. We conclude our literature account with a brief experimental outline, as well as with some therapeutic perspectives of our pharmacological hypothesis, that is that adrenal βarrestin1 is a novel molecular target for preventing tobacco-induced hyperaldosteronism, thereby also ameliorating tobacco-related heart disease development.
Keywords: adrenal cortex; aldosterone; angiotensin II; nicotine; tobacco–related heart disease; βarrestin.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Erratum: Eyestalk Ablation to Increase Ovarian Maturation in Mud Crabs.J Vis Exp. 2023 May 26;(195). doi: 10.3791/6561. J Vis Exp. 2023. PMID: 37235796
-
Depressing time: Waiting, melancholia, and the psychoanalytic practice of care.In: Kirtsoglou E, Simpson B, editors. The Time of Anthropology: Studies of Contemporary Chronopolitics. Abingdon: Routledge; 2020. Chapter 5. In: Kirtsoglou E, Simpson B, editors. The Time of Anthropology: Studies of Contemporary Chronopolitics. Abingdon: Routledge; 2020. Chapter 5. PMID: 36137063 Free Books & Documents. Review.
-
Interventions to reduce harm from continued tobacco use.Cochrane Database Syst Rev. 2016 Oct 13;10(10):CD005231. doi: 10.1002/14651858.CD005231.pub3. Cochrane Database Syst Rev. 2016. PMID: 27734465 Free PMC article. Review.
-
Correlation between cervical carcinogenesis and tobacco use by sexual partners.Hell J Nucl Med. 2019 Sep-Dec;22 Suppl 2:184-190. Hell J Nucl Med. 2019. PMID: 31802062
-
Body Image Distortion (Archived).2023 Sep 4. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Sep 4. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31536191 Free Books & Documents.
Cited by
-
Nicotine Diminishes Alpha2-Adrenergic Receptor-Dependent Protection Against Oxidative Stress in H9c2 Cardiomyocytes.Drug Des Devel Ther. 2024 Jan 12;18:71-80. doi: 10.2147/DDDT.S432453. eCollection 2024. Drug Des Devel Ther. 2024. PMID: 38229917 Free PMC article.
-
An integral perspective of canonical cigarette and e-cigarette-related cardiovascular toxicity based on the adverse outcome pathway framework.J Adv Res. 2023 Jun;48:227-257. doi: 10.1016/j.jare.2022.08.012. Epub 2022 Aug 21. J Adv Res. 2023. PMID: 35998874 Free PMC article. Review.
-
Nicotine-induced adrenal beta-arrestin1 upregulation mediates tobacco-related hyperaldosteronism leading to cardiac dysfunction.World J Cardiol. 2020 May 26;12(5):192-202. doi: 10.4330/wjc.v12.i5.192. World J Cardiol. 2020. PMID: 32547713 Free PMC article.
-
Impact of Aldosterone on the Failing Myocardium: Insights from Mitochondria and Adrenergic Receptors Signaling and Function.Cells. 2021 Jun 19;10(6):1552. doi: 10.3390/cells10061552. Cells. 2021. PMID: 34205363 Free PMC article. Review.
-
Role of aldosterone and mineralocorticoid receptor (MR) in addiction: A scoping review.Neurosci Biobehav Rev. 2023 Nov;154:105427. doi: 10.1016/j.neubiorev.2023.105427. Epub 2023 Oct 17. Neurosci Biobehav Rev. 2023. PMID: 37858908 Free PMC article.
References
-
- Connell JM, Davies E. The new biology of aldosterone. J Endocrinol. 2005;186:1‐20. - PubMed
-
- Marney AM, Brown NJ. Aldosterone and end‐organ damage. Clin Sci (Lond). 2007;113:267‐278. - PubMed
-
- Weber KT. Aldosterone in congestive heart failure. N Engl J Med. 2001;345:1689‐1697. - PubMed
-
- Zhao W, Ahokas RA, Weber KT, Sun Y. ANG II‐induced cardiac molecular and cellular events: role of aldosterone. Am J Physiol Heart Circ Physiol. 2006;291:H336‐343. - PubMed
-
- Swedberg K, Eneroth P, Kjekshus J, Wilhelmsen L. Hormones regulating cardiovascular function in patients with severe congestive heart failure and their relation to mortality. CONSENSUS Trial Study Group. Circulation. 1990;82:1730‐1736. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
