

The demographic and treatment options for patients with large cell neuroendocrine carcinoma of the lung
- PMID: 31087628
- PMCID: PMC6558599
- DOI: 10.1002/cam4.2188
The demographic and treatment options for patients with large cell neuroendocrine carcinoma of the lung
Abstract
Introduction: Lung large cell neuroendocrine carcinoma (L-LCNEC) is a rare, aggressive tumor, for which the optimal treatment strategies for LCNEC have not yet been established. In order to explore how to improve the outcome of prognosis for patients with LCNEC, this study investigated the effect of different treatments based on the data obtained from the Surveillance, Epidemiology, and End Results (SEER) database.
Methods: A total of 2594 LCNEC cases with conditional information were extracted from SEER database. Propensity Score Matching (PSM) method was conducted to reduce possible bias between groups. One-way ANOVA was used to test the differences of characteristics between groups. Univariate and multivariate Cox proportional hazard models were applied to identify prognostic factors.
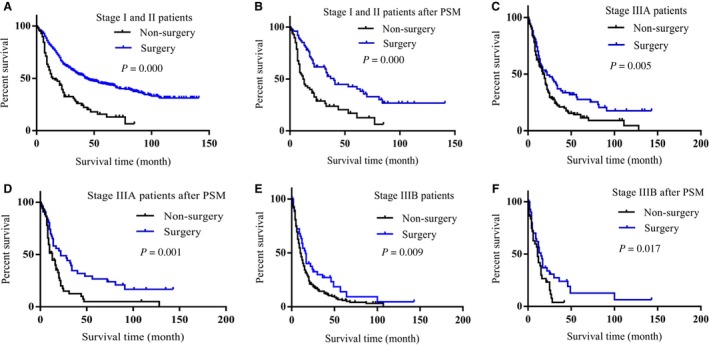
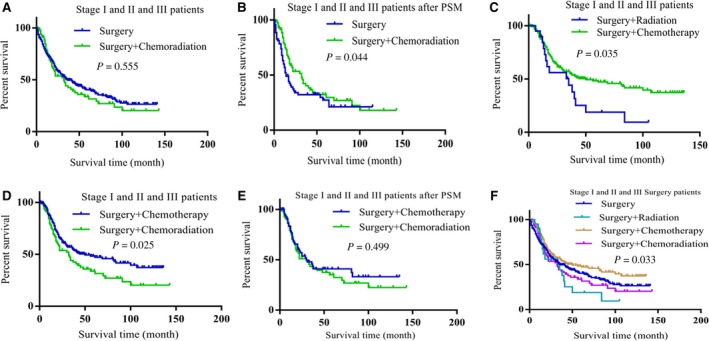
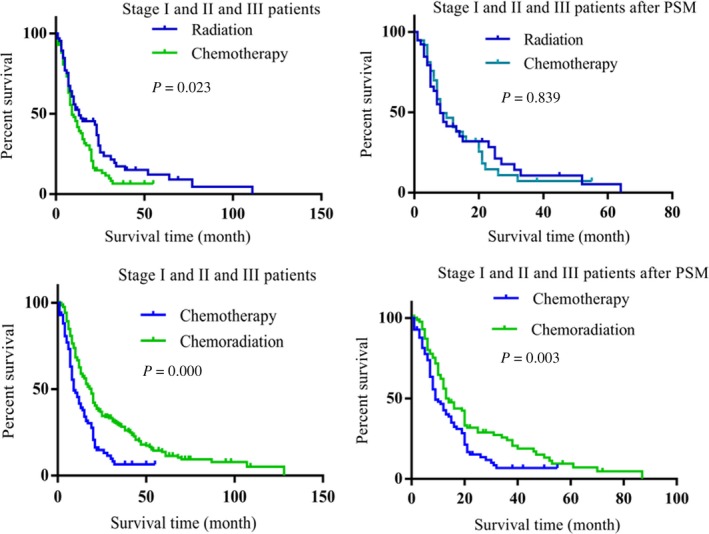
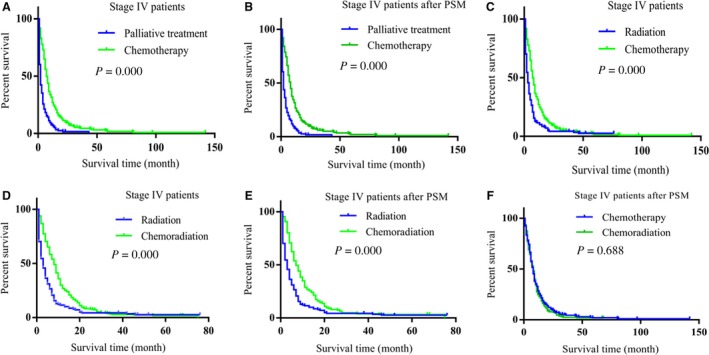
Results: Clinicopathologic characteristics including gender, age, TNM stage, T stage, N stage, and M stage were all identified as independent prognostic factors. Surgery benefited stage I, II, and III LCNEC patients' prognoses. The combination treatment that surgery combining with chemotherapy was the optimal treatment for stage I, II, and III LCENC patients. Compared with palliative treatment, stage IV patients obtained better prognoses with the treatment of radiation, chemotherapy, or chemoradiation. When comparing the effect of the three treatments (radiation, chemotherapy, and chemoradiation) in achieving better prognosis for stage IV patients, chemotherapy alone was better than the other treatments.
Conclusion: Surgery combining with chemotherapy was the optimal treatment for stage I, II, and III LCNEC patients; chemotherapy alone achieves more benefit than the other treatments for stage IV patients.
Keywords: chemotherapy; large cell neuroendocrine carcinoma; prognosis; radiation; surgery.
© 2019 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
There is no conflict of interest in this manuscript.
Figures
Similar articles
-
Incidence, survival comparison, and novel prognostic evaluation approaches for stage iii-iv pulmonary large cell neuroendocrine carcinoma and small cell lung cancer.BMC Cancer. 2023 Apr 5;23(1):312. doi: 10.1186/s12885-023-10797-3. BMC Cancer. 2023. PMID: 37020179 Free PMC article.
-
Clinicopathological characteristics and prognostic factors of pulmonary large cell neuroendocrine carcinoma: A large population-based analysis.Thorac Cancer. 2019 Apr;10(4):751-760. doi: 10.1111/1759-7714.12993. Epub 2019 Feb 7. Thorac Cancer. 2019. PMID: 30734490 Free PMC article.
-
Pulmonary large cell neuroendocrine carcinoma (LCNEC): a population-based study addressing recent molecular-genetic advances and emerging therapeutic approaches.Clin Exp Med. 2023 Nov;23(7):3947-3955. doi: 10.1007/s10238-023-01071-8. Epub 2023 Apr 15. Clin Exp Med. 2023. PMID: 37060529
-
Pathological features, clinical presentations and prognostic factors of ovarian large cell neuroendocrine carcinoma: a case report and review of published literature.J Ovarian Res. 2019 Jul 25;12(1):69. doi: 10.1186/s13048-019-0543-z. J Ovarian Res. 2019. PMID: 31345245 Free PMC article. Review.
-
Large cell neuroendocrine carcinoma of the lungs: case report and literature review.Ann Palliat Med. 2020 Sep;9(5):3705-3709. doi: 10.21037/apm-20-1667. Ann Palliat Med. 2020. PMID: 33065807 Review.
Cited by
-
Prognostic nomograms for lung neuroendocrine carcinomas based on lymph node ratio: a SEER database analysis.J Int Med Res. 2022 Sep;50(9):3000605221115160. doi: 10.1177/03000605221115160. J Int Med Res. 2022. PMID: 36076355 Free PMC article.
-
A prognostic nomogram based on least absolute shrinkage and selection operator Cox regression in patients with pulmonary large-cell neuroendocrine carcinoma.Transl Cancer Res. 2024 Feb 29;13(2):916-934. doi: 10.21037/tcr-23-1061. Epub 2024 Jan 24. Transl Cancer Res. 2024. PMID: 38482439 Free PMC article.
-
[Advances of Treatment of Pulmonary Large Cell Neuroendocrine Carcinoma].Zhongguo Fei Ai Za Zhi. 2024 Aug 20;27(8):622-628. doi: 10.3779/j.issn.1009-3419.2024.102.28. Zhongguo Fei Ai Za Zhi. 2024. PMID: 39318255 Free PMC article. Review. Chinese.
-
Survival outcomes of surgery in patients with pulmonary large-cell neuroendocrine carcinoma: a retrospective single-institution analysis and literature review.Orphanet J Rare Dis. 2021 Feb 12;16(1):82. doi: 10.1186/s13023-021-01730-7. Orphanet J Rare Dis. 2021. PMID: 33579331 Free PMC article. Review.
-
68Ga-Tetraazacyclododecane Tetraacetic Acid-DPhe1-Tyr3-Octreotate Positron Emission Tomography/Computed Tomographic Findings of Large-Cell Neuroendocrine Carcinoma of the Lung in a Child.Indian J Nucl Med. 2022 Oct-Dec;37(4):396-397. doi: 10.4103/ijnm.ijnm_50_22. Epub 2022 Dec 2. Indian J Nucl Med. 2022. PMID: 36817203 Free PMC article.
References
-
- Kawase A, Nagai K. Treatment strategy for neuroendocrine carcinoma of the lung. Gan To Kagaku Ryoho. 2009;36:1619‐1622. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
