

Targeting LIF-mediated paracrine interaction for pancreatic cancer therapy and monitoring
- PMID: 30996350
- PMCID: PMC6565370
- DOI: 10.1038/s41586-019-1130-6
Targeting LIF-mediated paracrine interaction for pancreatic cancer therapy and monitoring
Erratum in
-
Author Correction: Targeting LIF-mediated paracrine interaction for pancreatic cancer therapy and monitoring.Nature. 2021 Dec;600(7889):E18. doi: 10.1038/s41586-021-04176-w. Nature. 2021. PMID: 34848876 No abstract available.
Abstract
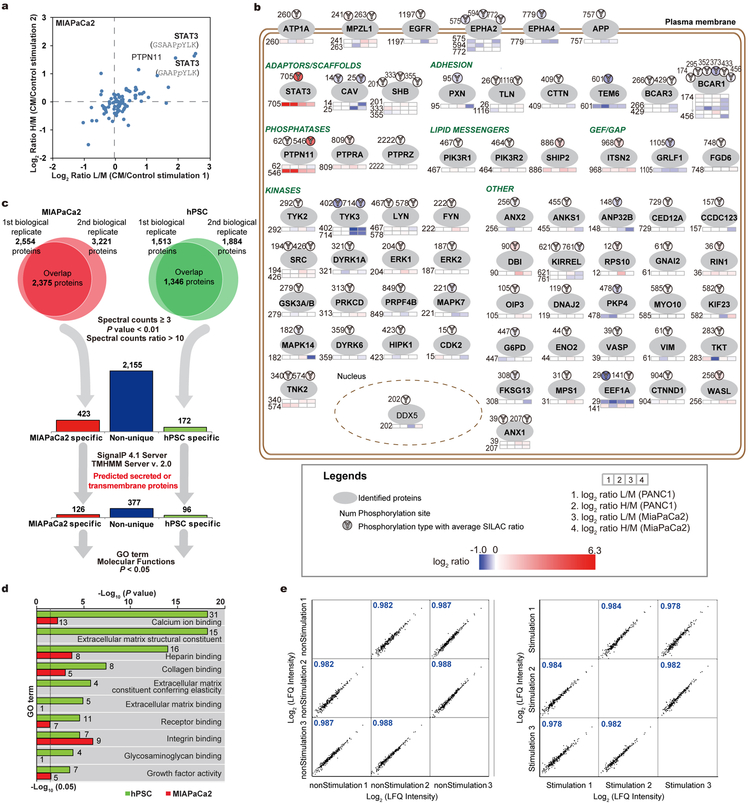
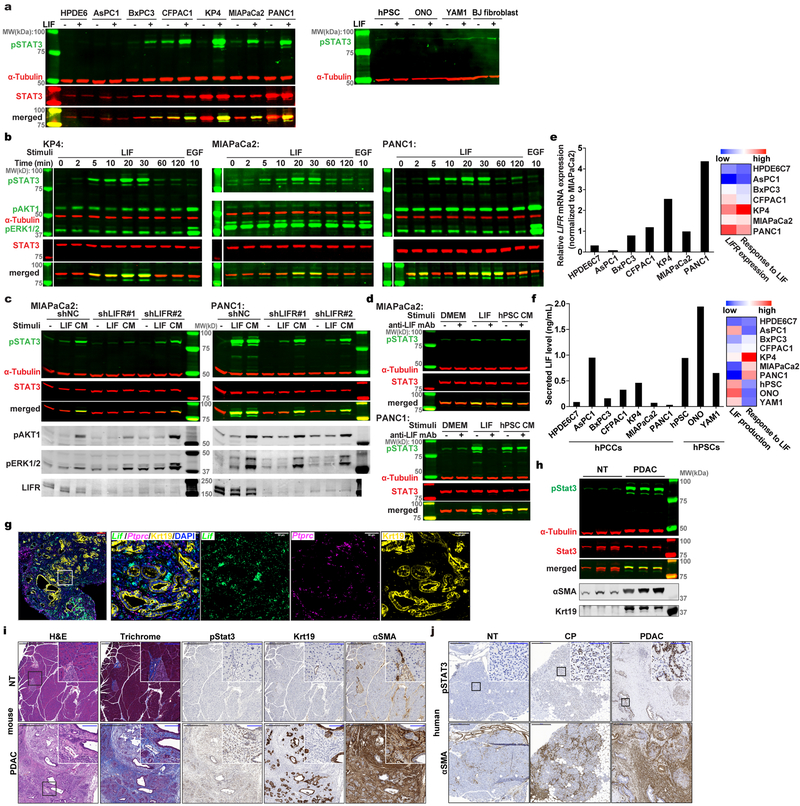
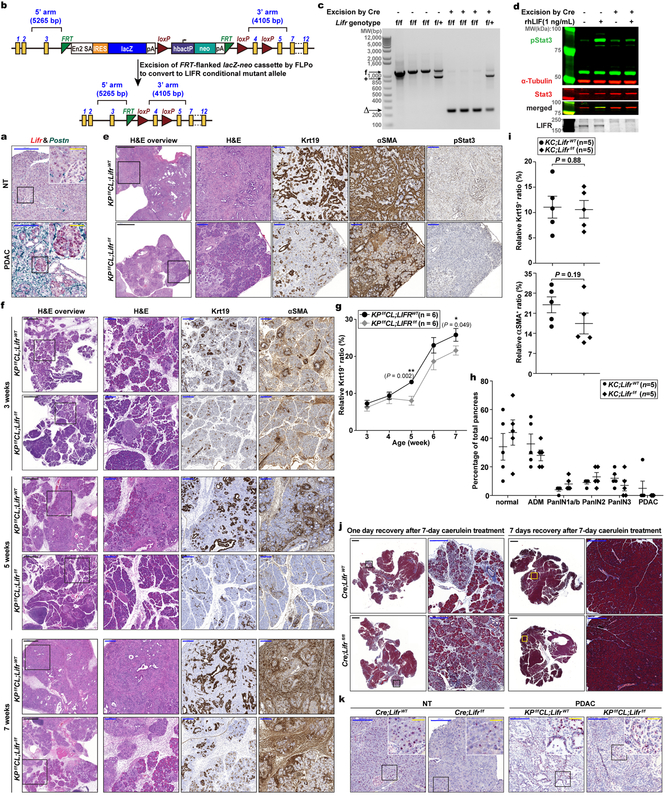
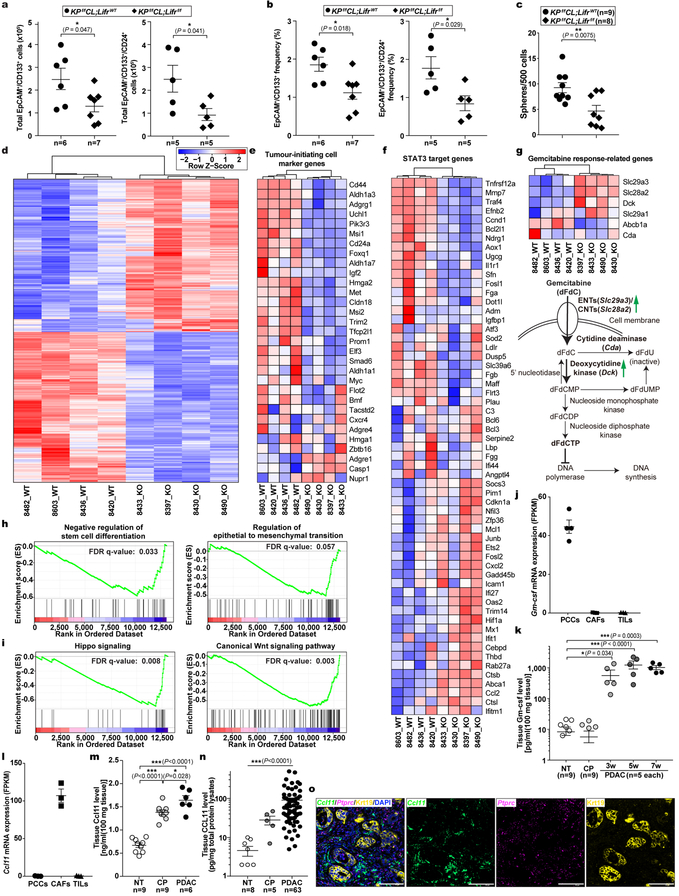
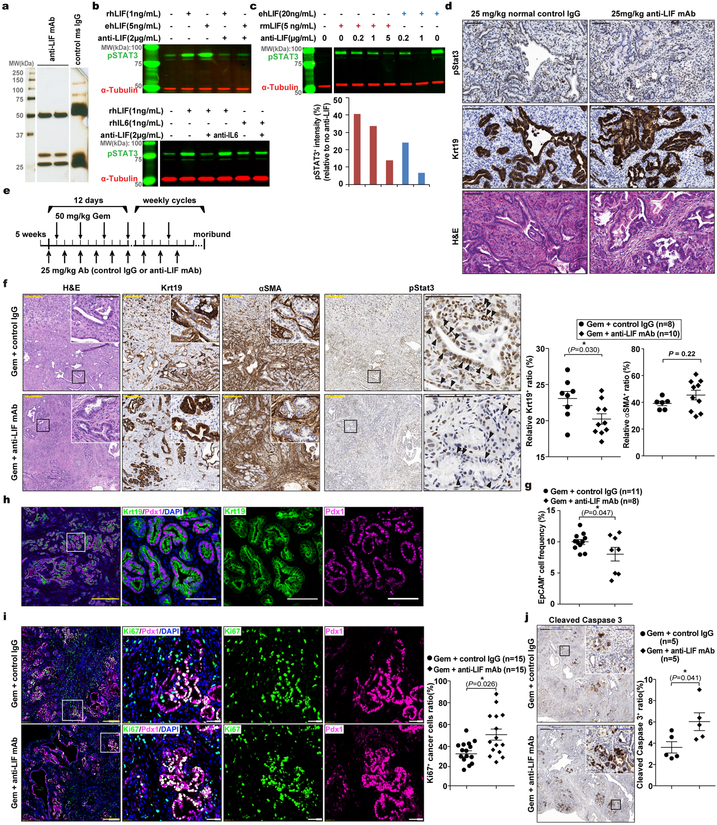
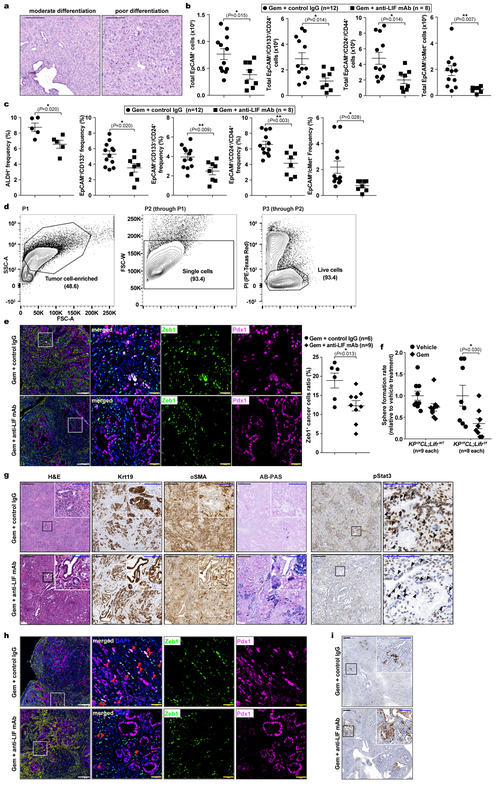
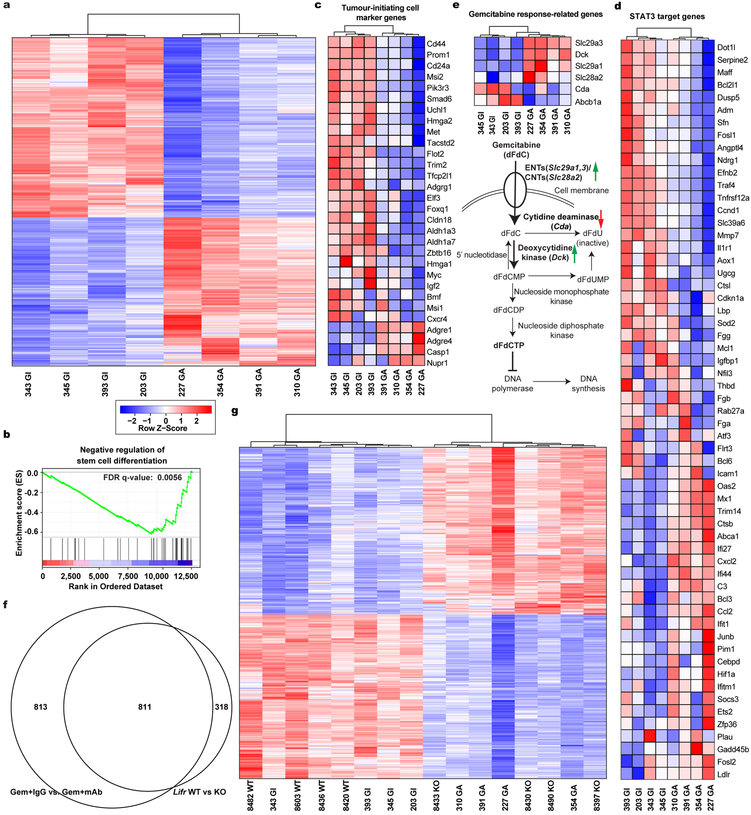
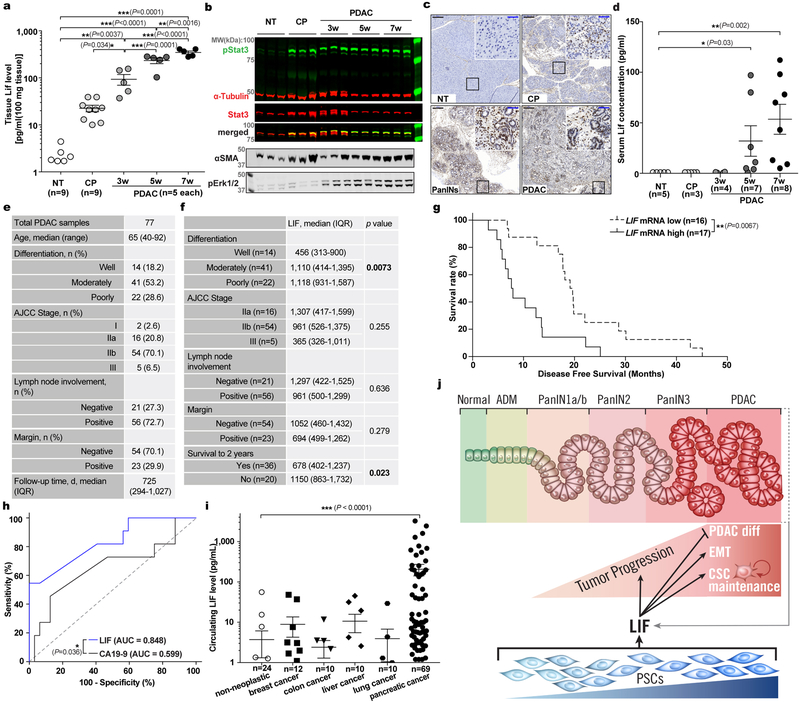
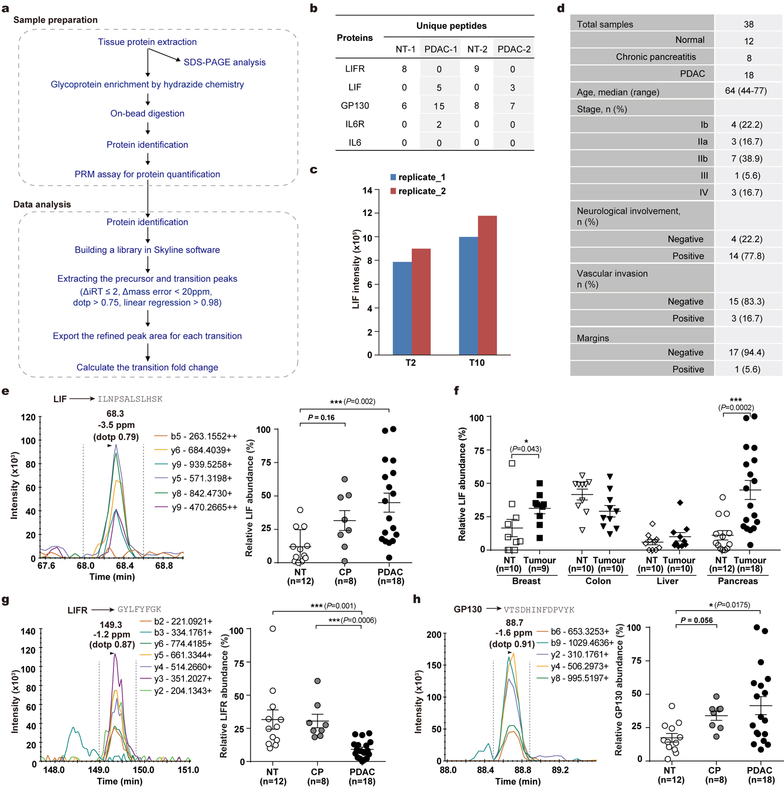
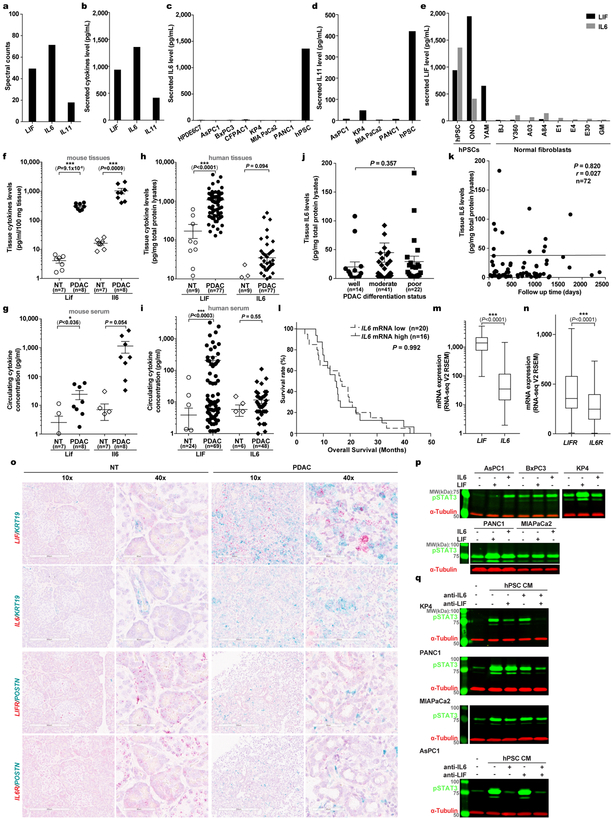
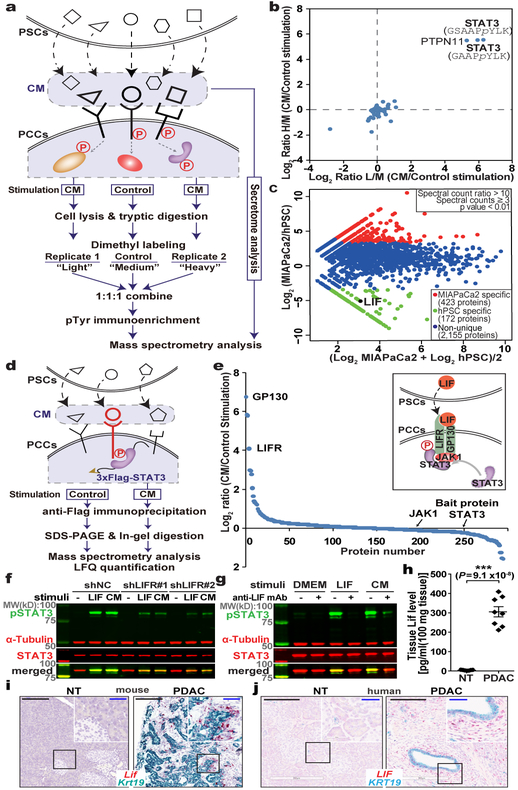
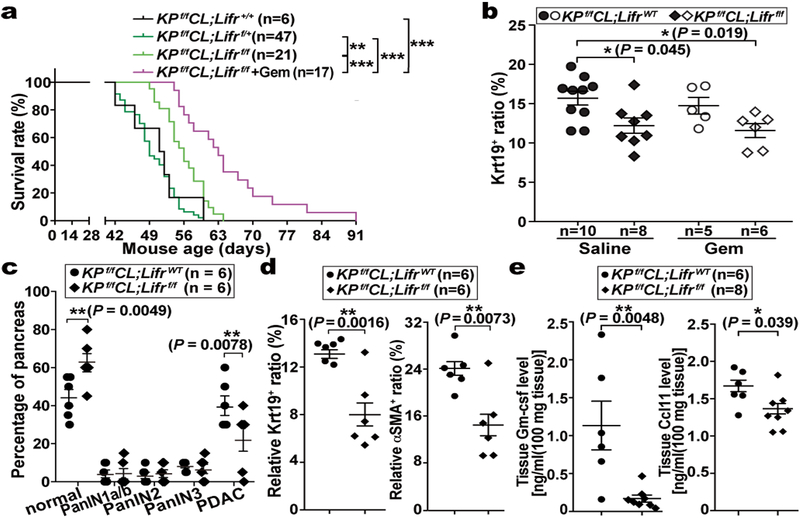
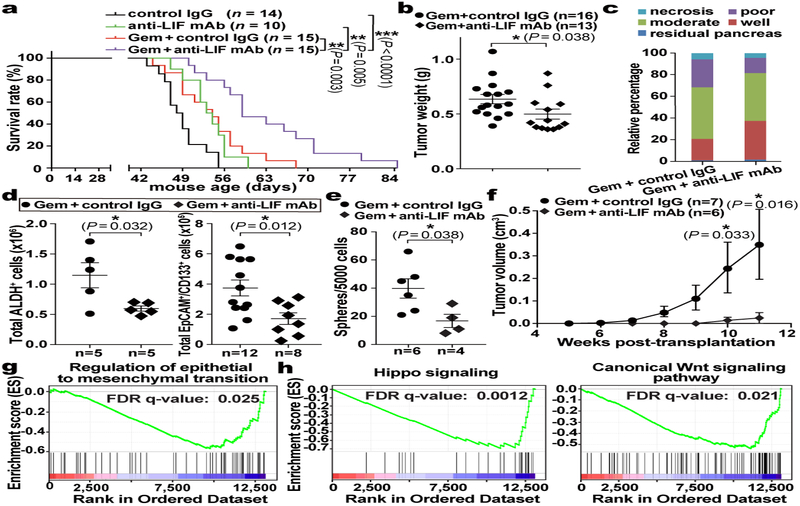
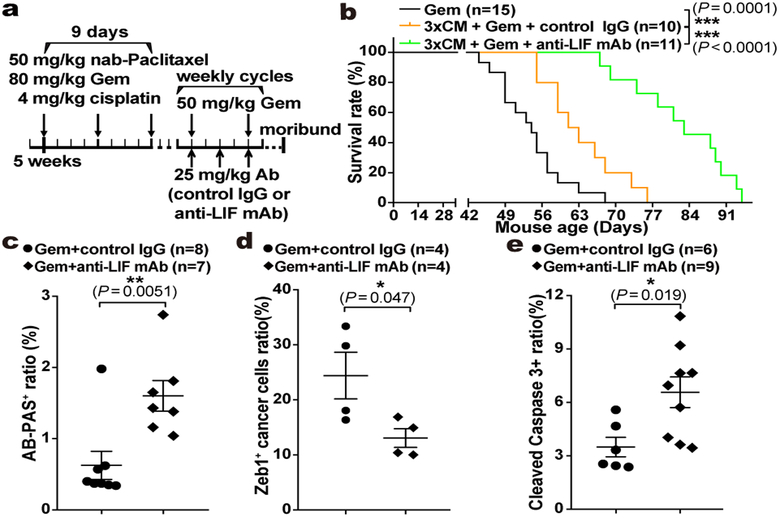
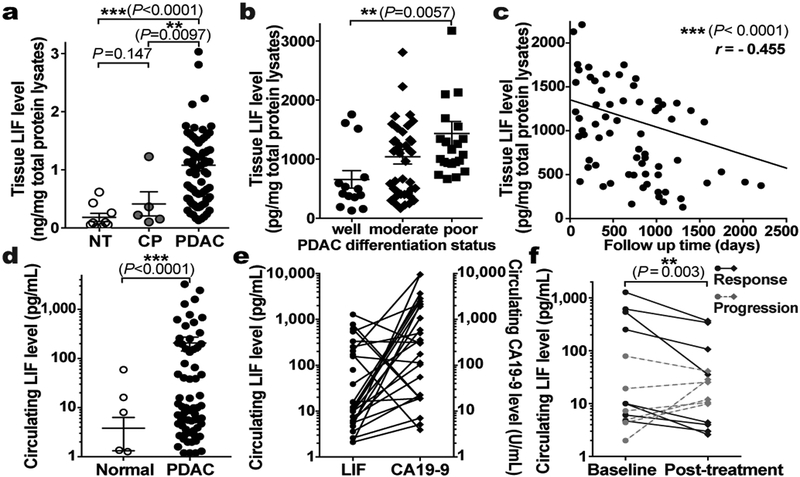
Pancreatic ductal adenocarcinoma (PDAC) has a dismal prognosis largely owing to inefficient diagnosis and tenacious drug resistance. Activation of pancreatic stellate cells (PSCs) and consequent development of dense stroma are prominent features accounting for this aggressive biology1,2. The reciprocal interplay between PSCs and pancreatic cancer cells (PCCs) not only enhances tumour progression and metastasis but also sustains their own activation, facilitating a vicious cycle to exacerbate tumorigenesis and drug resistance3-7. Furthermore, PSC activation occurs very early during PDAC tumorigenesis8-10, and activated PSCs comprise a substantial fraction of the tumour mass, providing a rich source of readily detectable factors. Therefore, we hypothesized that the communication between PSCs and PCCs could be an exploitable target to develop effective strategies for PDAC therapy and diagnosis. Here, starting with a systematic proteomic investigation of secreted disease mediators and underlying molecular mechanisms, we reveal that leukaemia inhibitory factor (LIF) is a key paracrine factor from activated PSCs acting on cancer cells. Both pharmacologic LIF blockade and genetic Lifr deletion markedly slow tumour progression and augment the efficacy of chemotherapy to prolong survival of PDAC mouse models, mainly by modulating cancer cell differentiation and epithelial-mesenchymal transition status. Moreover, in both mouse models and human PDAC, aberrant production of LIF in the pancreas is restricted to pathological conditions and correlates with PDAC pathogenesis, and changes in the levels of circulating LIF correlate well with tumour response to therapy. Collectively, these findings reveal a function of LIF in PDAC tumorigenesis, and suggest its translational potential as an attractive therapeutic target and circulating marker. Our studies underscore how a better understanding of cell-cell communication within the tumour microenvironment can suggest novel strategies for cancer therapy.
Conflict of interest statement
Figures
Similar articles
-
Repositioning Mifepristone as a Leukaemia Inhibitory Factor Receptor Antagonist for the Treatment of Pancreatic Adenocarcinoma.Cells. 2022 Nov 3;11(21):3482. doi: 10.3390/cells11213482. Cells. 2022. PMID: 36359879 Free PMC article.
-
Blockade of leukemia inhibitory factor as a therapeutic approach to KRAS driven pancreatic cancer.Nat Commun. 2019 Jul 11;10(1):3055. doi: 10.1038/s41467-019-11044-9. Nat Commun. 2019. PMID: 31296870 Free PMC article.
-
The critical roles of activated stellate cells-mediated paracrine signaling, metabolism and onco-immunology in pancreatic ductal adenocarcinoma.Mol Cancer. 2018 Feb 19;17(1):62. doi: 10.1186/s12943-018-0815-z. Mol Cancer. 2018. PMID: 29458370 Free PMC article. Review.
-
Galectin-3 Mediates Tumor Cell-Stroma Interactions by Activating Pancreatic Stellate Cells to Produce Cytokines via Integrin Signaling.Gastroenterology. 2018 Apr;154(5):1524-1537.e6. doi: 10.1053/j.gastro.2017.12.014. Epub 2017 Dec 21. Gastroenterology. 2018. PMID: 29274868
-
Pancreatic stellate cells and pancreas cancer: current perspectives and future strategies.Eur J Cancer. 2014 Oct;50(15):2570-82. doi: 10.1016/j.ejca.2014.06.021. Epub 2014 Aug 1. Eur J Cancer. 2014. PMID: 25091797 Review.
Cited by
-
KRAS-Driven Tumorigenesis and KRAS-Driven Therapy in Pancreatic Adenocarcinoma.Mol Cancer Ther. 2024 Oct 1;23(10):1378-1388. doi: 10.1158/1535-7163.MCT-23-0519. Mol Cancer Ther. 2024. PMID: 39118358 Review.
-
Stem Cell Factor LIFted as a Promising Clinical Target for Cancer Therapy.Mol Cancer Ther. 2019 Aug;18(8):1337-1340. doi: 10.1158/1535-7163.MCT-19-0605. Mol Cancer Ther. 2019. PMID: 31371576 Free PMC article. No abstract available.
-
A targetable LIFR-NF-κB-LCN2 axis controls liver tumorigenesis and vulnerability to ferroptosis.Nat Commun. 2021 Dec 17;12(1):7333. doi: 10.1038/s41467-021-27452-9. Nat Commun. 2021. PMID: 34921145 Free PMC article.
-
Signaling in the Physiology and Pathophysiology of Pancreatic Stellate Cells - a Brief Review of Recent Advances.Front Physiol. 2020 Feb 14;11:78. doi: 10.3389/fphys.2020.00078. eCollection 2020. Front Physiol. 2020. PMID: 32116785 Free PMC article. Review.
-
Focus on Therapeutic Options for Surgically Resectable Pancreatic Adenocarcinoma Based on Novel Biomarkers.Curr Oncol. 2023 Jul 6;30(7):6462-6472. doi: 10.3390/curroncol30070475. Curr Oncol. 2023. PMID: 37504335 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
- R01 CA155620/CA/NCI NIH HHS/United States
- R01 CA082683/CA/NCI NIH HHS/United States
- HHMI/Howard Hughes Medical Institute/United States
- R01 CA186043/CA/NCI NIH HHS/United States
- T32 GM007752/GM/NIGMS NIH HHS/United States
- U01 CA210240/CA/NCI NIH HHS/United States
- F31 CA206416/CA/NCI NIH HHS/United States
- F32 CA217033/CA/NCI NIH HHS/United States
- R35 CA197687/CA/NCI NIH HHS/United States
- P30 CA014195/CA/NCI NIH HHS/United States
- R01 CA080100/CA/NCI NIH HHS/United States
- R01 CA227807/CA/NCI NIH HHS/United States
- P50 CA127297/CA/NCI NIH HHS/United States
- R50 CA211462/CA/NCI NIH HHS/United States
- R01 CA222862/CA/NCI NIH HHS/United States
- P30 CA036727/CA/NCI NIH HHS/United States
- R35 CA197699/CA/NCI NIH HHS/United States
- R01 CA178015/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
