

Modeling Regional Transmission and Containment of a Healthcare-associated Multidrug-resistant Organism
- PMID: 30919885
- PMCID: PMC6765447
- DOI: 10.1093/cid/ciz248
Modeling Regional Transmission and Containment of a Healthcare-associated Multidrug-resistant Organism
Abstract
Background: The Centers for Disease Control and Prevention (CDC) recently published interim guidance for a public health response to contain novel or targeted multidrug-resistant organisms (MDROs). We assessed the impact of implementing the strategy in a US state using a mathematical model.
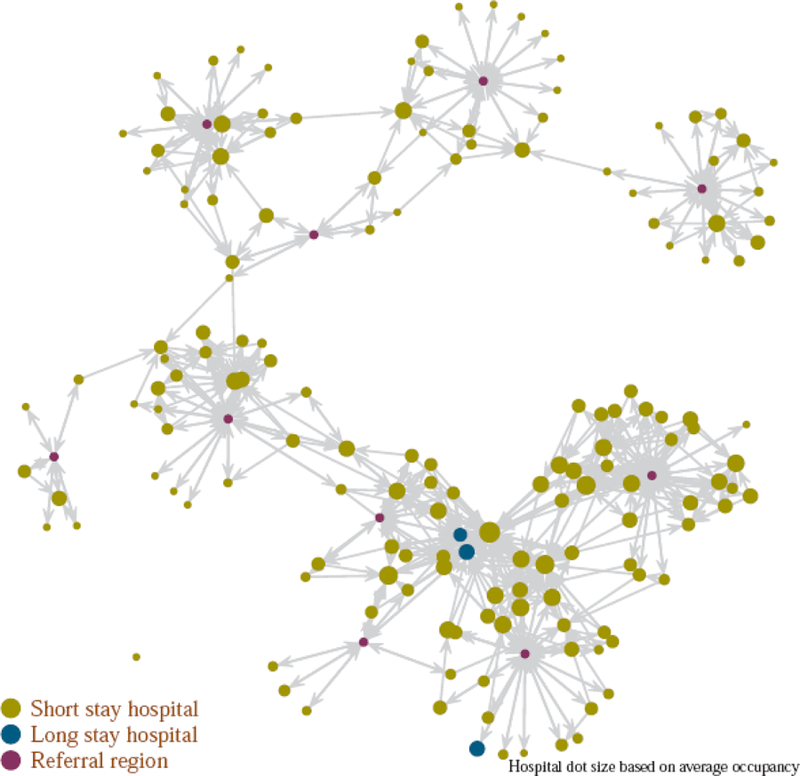
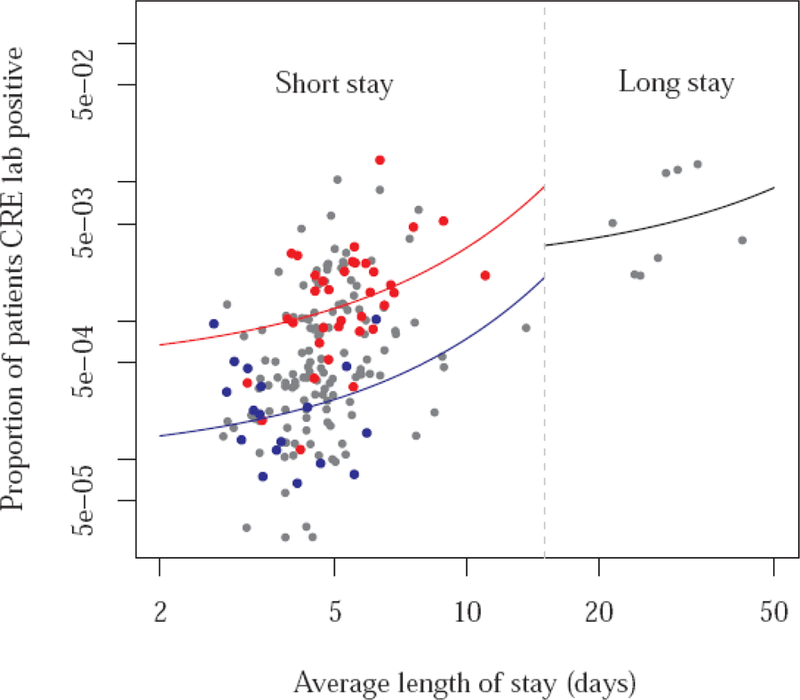
Methods: We used a deterministic compartmental model, parametrized via a novel analysis of carbapenem-resistant Enterobacteriaceae data reported to the National Healthcare Safety Network and patient transfer data from the Centers for Medicare and Medicaid Services. The simulations assumed that after the importation of the MDRO and its initial detection by clinical culture at an index hospital, fortnightly prevalence surveys for colonization and additional infection control interventions were implemented at the index facility; similar surveys were then also implemented at those facilities known to be connected most strongly to it as measured by patient transfer data; and prevalence surveys were discontinued after 2 consecutive negative surveys.
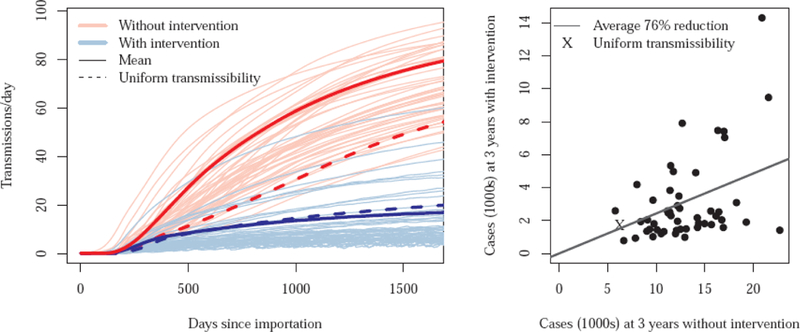
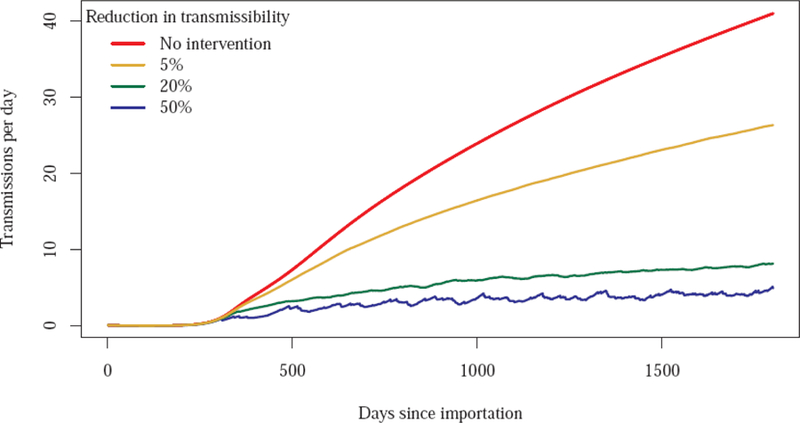
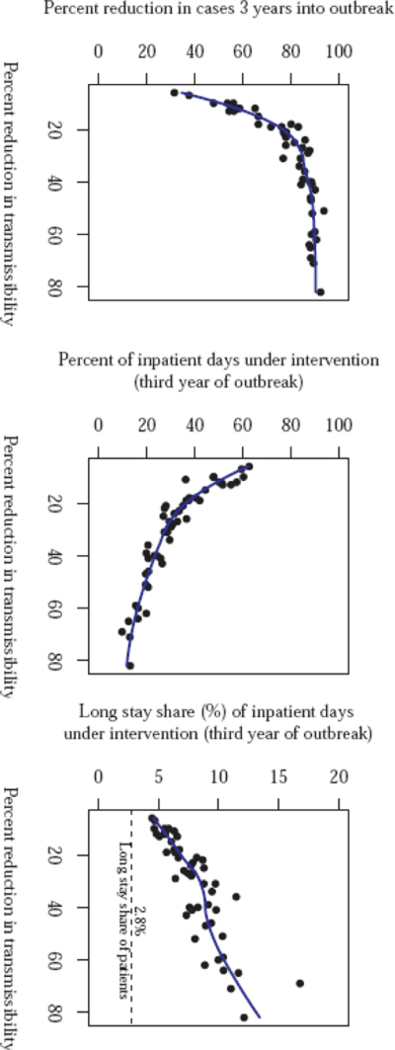
Results: If additional infection-control interventions are assumed to lead to a 20% reduction in transmissibility in intervention facilities, prevalent case count in the state 3 years after importation would be reduced by 76% (interquartile range: 73-77%). During the third year, these additional infection-control measures would be applied in facilities accounting for 42% (37-46%) of inpatient days.
Conclusions: CDC guidance for containing MDROs, when used in combination with information on transfer of patients among hospitals, is predicted to be effective, enabling targeted and efficient use of prevention resources during an outbreak response. Even modestly effective infection-control measures may lead to a substantial reduction in transmission events.
Keywords: healthcare epidemiology; mathematical model; multidrug-resistant organism.
Published by Oxford University Press for the Infectious Diseases Society of America 2019.
Conflict of interest statement
No authors have any potential conflicts of interest to disclose.
Figures
Similar articles
-
Regional impact of multidrug-resistant organism prevention bundles implemented by facility type: A modeling study.Infect Control Hosp Epidemiol. 2024 Jul;45(7):856-863. doi: 10.1017/ice.2023.278. Epub 2024 Feb 28. Infect Control Hosp Epidemiol. 2024. PMID: 38415308 Free PMC article.
-
Modeling Interventions to Reduce the Spread of Multidrug-Resistant Organisms Between Health Care Facilities in a Region.JAMA Netw Open. 2021 Aug 2;4(8):e2119212. doi: 10.1001/jamanetworkopen.2021.19212. JAMA Netw Open. 2021. PMID: 34347060 Free PMC article.
-
Infection control measures and prevalence of multidrug-resistant organisms in non-hospital care settings in northeastern Germany: results from a one-day point prevalence study.J Hosp Infect. 2017 Nov;97(3):234-240. doi: 10.1016/j.jhin.2017.08.002. Epub 2017 Aug 8. J Hosp Infect. 2017. PMID: 28797758
-
An integrative review of infection prevention and control programs for multidrug-resistant organisms in acute care hospitals: a socio-ecological perspective.Am J Infect Control. 2011 Jun;39(5):368-378. doi: 10.1016/j.ajic.2010.07.017. Epub 2011 Mar 23. Am J Infect Control. 2011. PMID: 21429622 Review.
-
Transmission pathways of multidrug-resistant organisms in the hospital setting: a scoping review.Infect Control Hosp Epidemiol. 2019 Apr;40(4):447-456. doi: 10.1017/ice.2018.359. Epub 2019 Mar 6. Infect Control Hosp Epidemiol. 2019. PMID: 30837029 Free PMC article. Review.
Cited by
-
Combating Antimicrobial Resistance: Going Beyond New Antibiotics.Clin Ther. 2020 Sep;42(9):1625-1627. doi: 10.1016/j.clinthera.2020.08.005. Epub 2020 Sep 9. Clin Ther. 2020. PMID: 32919753 Free PMC article. No abstract available.
-
Regional impact of multidrug-resistant organism prevention bundles implemented by facility type: A modeling study.Infect Control Hosp Epidemiol. 2024 Jul;45(7):856-863. doi: 10.1017/ice.2023.278. Epub 2024 Feb 28. Infect Control Hosp Epidemiol. 2024. PMID: 38415308 Free PMC article.
-
The importance of active surveillance of carbapenem-resistant Enterobacterales (CRE) in colonization rates in critically ill patients.PLoS One. 2022 Jan 20;17(1):e0262554. doi: 10.1371/journal.pone.0262554. eCollection 2022. PLoS One. 2022. PMID: 35051212 Free PMC article.
-
Challenges in Forecasting Antimicrobial Resistance.Emerg Infect Dis. 2023 Apr;29(4):679-685. doi: 10.3201/eid2904.221552. Emerg Infect Dis. 2023. PMID: 36958029 Free PMC article. Review.
-
System identifiability in a time-evolving agent-based model.PLoS One. 2024 Jan 25;19(1):e0290821. doi: 10.1371/journal.pone.0290821. eCollection 2024. PLoS One. 2024. PMID: 38271401 Free PMC article.
References
-
- Centers for Disease Control and Prevention. Tracking CRE Available at: https://www.cdc.gov/hai/organisms/cre/trackingcre.html Accessed May 15, 2018.
