

Active and passive case-finding in tuberculosis-affected households in Peru: a 10-year prospective cohort study
- PMID: 30910427
- PMCID: PMC6483977
- DOI: 10.1016/S1473-3099(18)30753-9
Active and passive case-finding in tuberculosis-affected households in Peru: a 10-year prospective cohort study
Abstract
Background: Active case-finding among contacts of patients with tuberculosis is a global health priority, but the effects of active versus passive case-finding are poorly characterised. We assessed the contribution of active versus passive case-finding to tuberculosis detection among contacts and compared sex and disease characteristics between contacts diagnosed through these strategies.
Methods: In shanty towns in Callao, Peru, we identified index patients with tuberculosis and followed up contacts aged 15 years or older for tuberculosis. All patients and contacts were offered free programmatic active case-finding entailing sputum smear microscopy and clinical assessment. Additionally, all contacts were offered intensified active case-finding with sputum smear and culture testing monthly for 6 months and then once every 4 years. Passive case-finding at local health facilities was ongoing throughout follow-up.
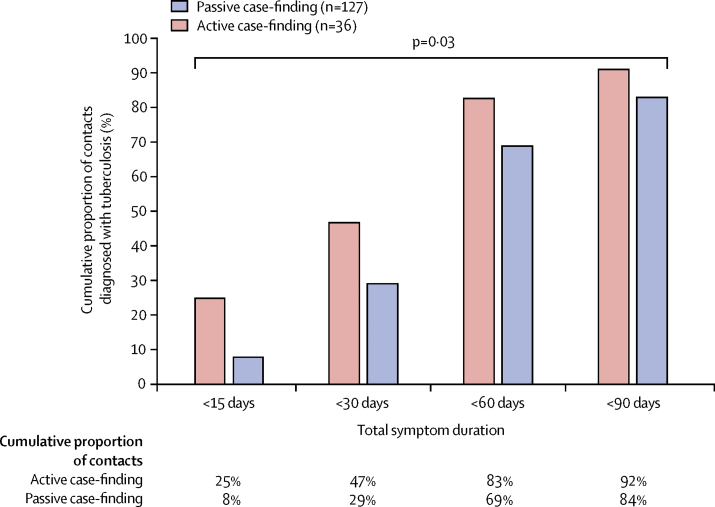
Findings: Between Oct 23, 2002, and May 26, 2006, we identified 2666 contacts, who were followed up until March 1, 2016. Median follow-up was 10·0 years (IQR 7·5-11·0). 232 (9%) of 2666 contacts were diagnosed with tuberculosis. The 2-year cumulative risk of tuberculosis was 4·6% (95% CI 3·5-5·5), and overall incidence was 0·98 cases (95% CI 0·86-1·10) per 100 person-years. 53 (23%) of 232 contacts with tuberculosis were diagnosed through active case-finding and 179 (77%) were identified through passive case-finding. During the first 6 months of the study, 23 (45%) of 51 contacts were diagnosed through active case-finding and 28 (55%) were identified through passive case-finding. Contacts diagnosed through active versus passive case-finding were more frequently female (36 [68%] of 53 vs 85 [47%] of 179; p=0·009), had a symptom duration of less than 15 days (nine [25%] of 36 vs ten [8%] of 127; p=0·03), and were more likely to be sputum smear-negative (33 [62%] of 53 vs 62 [35%] of 179; p=0·0003).
Interpretation: Although active case-finding made an important contribution to tuberculosis detection among contacts, passive case-finding detected most of the tuberculosis burden. Compared with passive case-finding, active case-finding was equitable, helped to diagnose tuberculosis earlier and usually before a positive result on sputum smear microscopy, and showed a high burden of undetected tuberculosis among women.
Funding: Wellcome Trust, Department for International Development Civil Society Challenge Fund, Joint Global Health Trials consortium, Bill & Melinda Gates Foundation, Imperial College National Institutes of Health Research Biomedical Research Centre, Foundation for Innovative New Diagnostics, Sir Halley Stewart Trust, WHO, TB REACH, and IFHAD: Innovation for Health and Development.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures





Comment in
-
Tuberculosis active case-finding: more than just finding cases.Lancet Infect Dis. 2019 May;19(5):456-457. doi: 10.1016/S1473-3099(19)30065-9. Epub 2019 Mar 22. Lancet Infect Dis. 2019. PMID: 30910430 No abstract available.
Similar articles
-
A score to predict and stratify risk of tuberculosis in adult contacts of tuberculosis index cases: a prospective derivation and external validation cohort study.Lancet Infect Dis. 2017 Nov;17(11):1190-1199. doi: 10.1016/S1473-3099(17)30447-4. Epub 2017 Aug 18. Lancet Infect Dis. 2017. PMID: 28827142 Free PMC article.
-
A household-level score to predict the risk of tuberculosis among contacts of patients with tuberculosis: a derivation and external validation prospective cohort study.Lancet Infect Dis. 2020 Jan;20(1):110-122. doi: 10.1016/S1473-3099(19)30423-2. Epub 2019 Oct 31. Lancet Infect Dis. 2020. PMID: 31678031 Free PMC article.
-
Expanding tuberculosis case detection by screening household contacts.Public Health Rep. 2005 May-Jun;120(3):271-7. doi: 10.1177/003335490512000309. Public Health Rep. 2005. PMID: 16134567 Free PMC article.
-
Tuberculosis.In: Holmes KK, Bertozzi S, Bloom BR, Jha P, editors. Major Infectious Diseases. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 3. Chapter 11. In: Holmes KK, Bertozzi S, Bloom BR, Jha P, editors. Major Infectious Diseases. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 3. Chapter 11. PMID: 30212088 Free Books & Documents. Review.
-
Active case finding in contacts of people with tuberculosis.Cochrane Database Syst Rev. 2011 Sep 7;2011(9):CD008477. doi: 10.1002/14651858.CD008477.pub2. Cochrane Database Syst Rev. 2011. PMID: 21901723 Free PMC article. Review.
Cited by
-
Tuberculosis Case Finding in Kulon Progo District, Yogyakarta, Indonesia: Passive versus Active Case Finding Using Mobile Chest X-ray.Trop Med Infect Dis. 2024 Apr 4;9(4):75. doi: 10.3390/tropicalmed9040075. Trop Med Infect Dis. 2024. PMID: 38668536 Free PMC article.
-
Analysis on time delay of tuberculosis among adolescents and young adults in Eastern China.Front Public Health. 2024 Apr 8;12:1376404. doi: 10.3389/fpubh.2024.1376404. eCollection 2024. Front Public Health. 2024. PMID: 38651131 Free PMC article.
-
Improving tuberculosis case detection through contact risk stratification by Xpert MTB/RIF Ultra and spatial parameters: Evaluation of an innovative active case finding strategy in Mozambique (Xpatial-TB).PLOS Glob Public Health. 2024 Feb 9;4(2):e0002789. doi: 10.1371/journal.pgph.0002789. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 38335231 Free PMC article.
-
Improving TB Case Detection Through Active Case-Finding: Results of Multiple Intervention Strategies in Hard-to-Reach Riverine Areas of Southern Nigeria.Glob Health Sci Pract. 2024 Feb 28;12(1):e2300164. doi: 10.9745/GHSP-D-23-00164. Print 2024 Feb 28. Glob Health Sci Pract. 2024. PMID: 38290754 Free PMC article.
-
Facilitators and barriers to tuberculosis active case findings in low- and middle-income countries: a systematic review of qualitative research.BMC Infect Dis. 2023 Aug 7;23(1):515. doi: 10.1186/s12879-023-08502-7. BMC Infect Dis. 2023. PMID: 37550614 Free PMC article.
References
-
- WHO . World Health Organization; Geneva: 2018. Global tuberculosis report 2018.
-
- WHO . World Health Organization; Geneva: 2018. Latent tuberculosis infection: updated and consolidated guidelines for programmatic management. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
