

Global burden of maternal and congenital syphilis and associated adverse birth outcomes-Estimates for 2016 and progress since 2012
- PMID: 30811406
- PMCID: PMC6392238
- DOI: 10.1371/journal.pone.0211720
Global burden of maternal and congenital syphilis and associated adverse birth outcomes-Estimates for 2016 and progress since 2012
Erratum in
-
Correction: Global burden of maternal and congenital syphilis and associated adverse birth outcomes-Estimates for 2016 and progress since 2012.PLoS One. 2019 Jul 5;14(7):e0219613. doi: 10.1371/journal.pone.0219613. eCollection 2019. PLoS One. 2019. PMID: 31276484 Free PMC article.
Abstract
Background: In 2007 the World Health Organization (WHO) launched the global initiative to eliminate mother-to-child transmission of syphilis (congenital syphilis, or CS). To assess progress towards the goal of <50 CS cases per 100,000 live births, we generated regional and global estimates of maternal and congenital syphilis for 2016 and updated the 2012 estimates.
Methods: Maternal syphilis estimates were generated using the Spectrum-STI model, fitted to sentinel surveys and routine testing of pregnant women during antenatal care (ANC) and other representative population data. Global and regional estimates of CS used the same approach as previous WHO estimates.
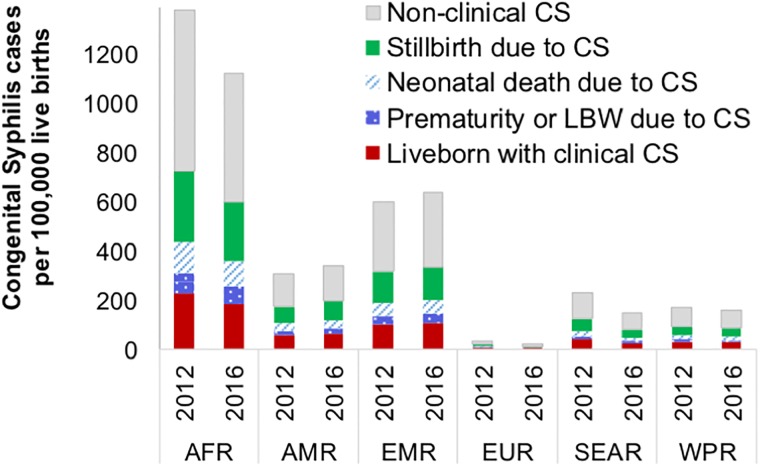
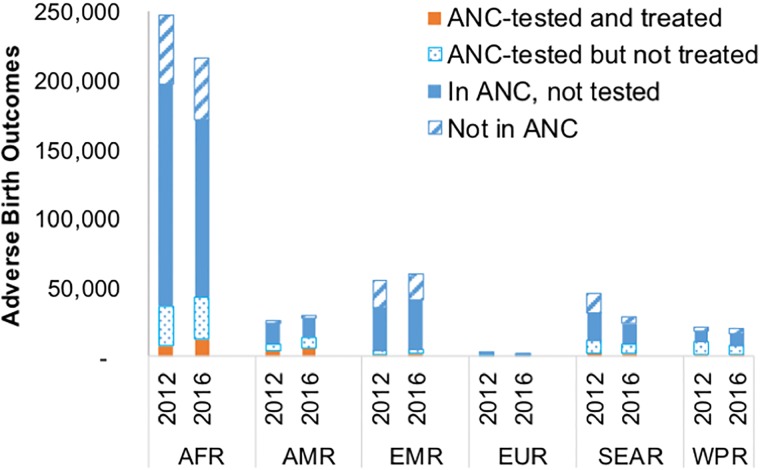
Results: The estimated global maternal syphilis prevalence in 2016 was 0.69% (95% confidence interval: 0.57-0.81%) resulting in a global CS rate of 473 (385-561) per 100,000 live births and 661,000 (538,000-784,000) total CS cases, including 355,000 (290,000-419,000) adverse birth outcomes (ABO) and 306,000 (249,000-363,000) non-clinical CS cases (infants without clinical signs born to un-treated mothers). The ABOs included 143,000 early fetal deaths and stillbirths, 61,000 neonatal deaths, 41,000 preterm or low-birth weight births, and 109,000 infants with clinical CS. Of these ABOs- 203,000 (57%) occurred in pregnant women attending ANC but not screened for syphilis; 74,000 (21%) in mothers not enrolled in ANC, 55,000 (16%) in mothers screened but not treated, and 23,000 (6%) in mothers enrolled, screened and treated. The revised 2012 estimates were 0.70% (95% CI: 0.63-0.77%) maternal prevalence, and 748,000 CS cases (539 per 100,000 live births) including 397,000 (361,000-432,000) ABOs. The estimated decrease in CS case rates between 2012 and 2016 reflected increased access to ANC and to syphilis screening and treatment.
Conclusions: Congenital syphilis decreased worldwide between 2012 and 2016, although maternal prevalence was stable. Achieving global CS elimination, however, will require improving access to early syphilis screening and treatment in ANC, clinically monitoring all women diagnosed with syphilis and their infants, improving partner management, and reducing syphilis prevalence in the general population by expanding testing, treatment and partner referral beyond ANC.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Global burden of maternal and congenital syphilis in 2008 and 2012: a health systems modelling study.Lancet Glob Health. 2016 Aug;4(8):e525-33. doi: 10.1016/S2214-109X(16)30135-8. Lancet Glob Health. 2016. PMID: 27443780 Free PMC article.
-
Global estimates of syphilis in pregnancy and associated adverse outcomes: analysis of multinational antenatal surveillance data.PLoS Med. 2013;10(2):e1001396. doi: 10.1371/journal.pmed.1001396. Epub 2013 Feb 26. PLoS Med. 2013. PMID: 23468598 Free PMC article.
-
Estimating the Public Health Burden Associated With Adverse Pregnancy Outcomes Resulting From Syphilis Infection Across 43 Countries in Sub-Saharan Africa.Sex Transm Dis. 2015 Jul;42(7):369-75. doi: 10.1097/OLQ.0000000000000291. Sex Transm Dis. 2015. PMID: 26222749 Free PMC article.
-
Reaching beyond pregnant women to eliminate mother-to-child transmission of syphilis in Africa.Expert Rev Anti Infect Ther. 2014 Jun;12(6):705-14. doi: 10.1586/14787210.2014.919221. Expert Rev Anti Infect Ther. 2014. PMID: 24834453 Review.
-
Untreated maternal syphilis and adverse outcomes of pregnancy: a systematic review and meta-analysis.Bull World Health Organ. 2013 Mar 1;91(3):217-26. doi: 10.2471/BLT.12.107623. Epub 2013 Jan 17. Bull World Health Organ. 2013. PMID: 23476094 Free PMC article. Review.
Cited by
-
The relationship between selected sexually transmitted pathogens, HPV and HIV infection status in women presenting with gynaecological symptoms in Maputo City, Mozambique.PLoS One. 2024 Sep 6;19(9):e0307781. doi: 10.1371/journal.pone.0307781. eCollection 2024. PLoS One. 2024. PMID: 39240843 Free PMC article.
-
Analysis of Adverse Pregnancy Outcomes of Pregnant Women with Syphilis and Maternal-Infant Serological Association in Changzhou, China, 2015-2019.Stem Cells Int. 2022 Sep 5;2022:9673850. doi: 10.1155/2022/9673850. eCollection 2022. Stem Cells Int. 2022. Retraction in: Stem Cells Int. 2023 Sep 14;2023:9879658. doi: 10.1155/2023/9879658. PMID: 36106175 Free PMC article. Retracted.
-
Seroprevalence of Hepatitis B Virus, Hepatitis C Virus, Syphilis and Associated Factors Among Female Sex Workers in Gondar Town, Northwest Ethiopia.Infect Drug Resist. 2022 Oct 14;15:5915-5927. doi: 10.2147/IDR.S380952. eCollection 2022. Infect Drug Resist. 2022. PMID: 36254334 Free PMC article.
-
Congenital Syphilis: a Review of Global Epidemiology.Clin Microbiol Rev. 2023 Jun 21;36(2):e0012622. doi: 10.1128/cmr.00126-22. Epub 2023 Mar 15. Clin Microbiol Rev. 2023. PMID: 36920205 Free PMC article. Review.
-
Differences in maternal characteristics and pregnancy outcomes between syphilitic women with and without partner coinfection.BMC Pregnancy Childbirth. 2019 Nov 27;19(1):439. doi: 10.1186/s12884-019-2569-z. BMC Pregnancy Childbirth. 2019. PMID: 31771540 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
