

Trends in Incidence of Methicillin-resistant Staphylococcus aureus Bloodstream Infections Differ by Strain Type and Healthcare Exposure, United States, 2005-2013
- PMID: 30801635
- PMCID: PMC6708714
- DOI: 10.1093/cid/ciz158
Trends in Incidence of Methicillin-resistant Staphylococcus aureus Bloodstream Infections Differ by Strain Type and Healthcare Exposure, United States, 2005-2013
Abstract
Background: Previous reports suggested that US methicillin-resistant Staphylococcus aureus (MRSA) strain epidemiology has changed since the rise of USA300 MRSA. We describe invasive MRSA trends by strain type.
Methods: Data came from 5 Centers for Disease Control and Prevention Emerging Infections Program sites conducting population-based surveillance and collecting isolates for invasive MRSA (ie, from normally sterile body sites), 2005-2013. MRSA bloodstream infection (BSI) incidence per 100 000 population was stratified by strain type and epidemiologic classification of healthcare exposures. Invasive USA100 vs USA300 case characteristics from 2013 were compared through logistic regression.
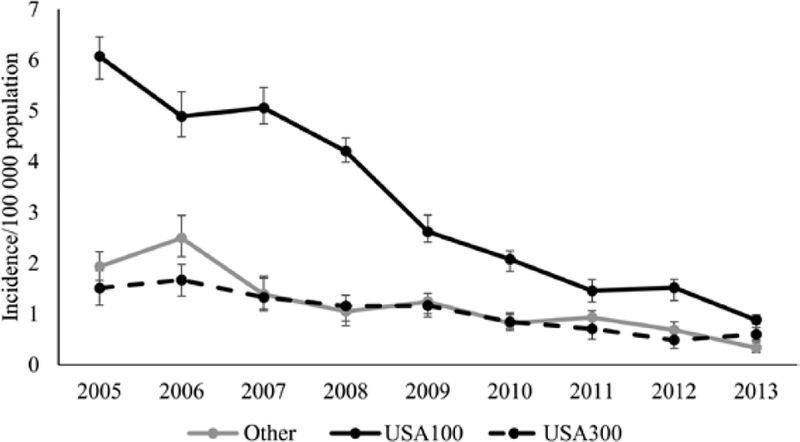
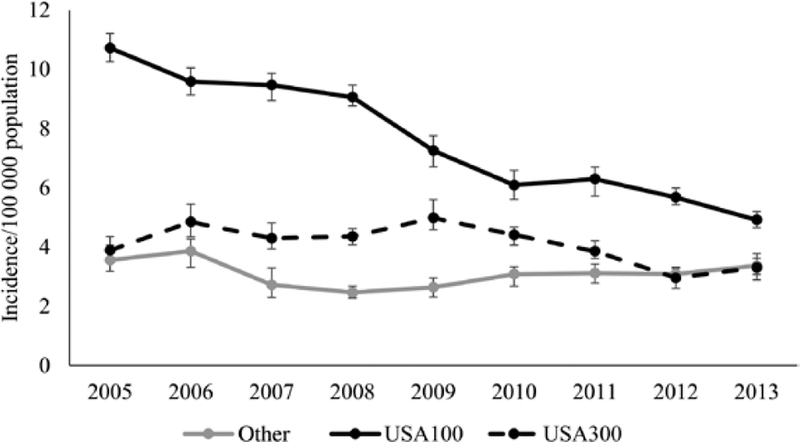
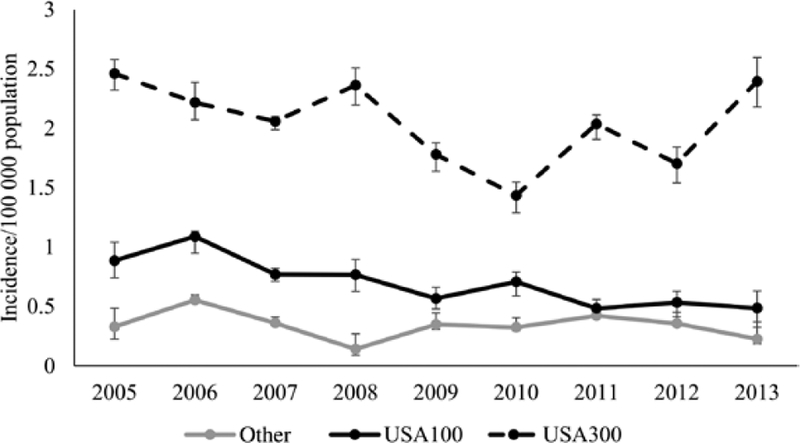
Results: From 2005 to 2013, USA100 incidence decreased most notably for hospital-onset (6.1 vs 0.9/100 000 persons, P < .0001) and healthcare-associated, community-onset (10.7 vs 4.9/100 000 persons, P < .0001) BSIs. USA300 incidence for hospital-onset BSIs also decreased (1.5 vs 0.6/100 000 persons, P < .0001). However, USA300 incidence did not significantly change for healthcare-associated, community-onset (3.9 vs 3.3/100 000 persons, P = .05) or community-associated BSIs (2.5 vs 2.4/100 000 persons, P = .19). Invasive MRSA was less likely to be USA300 in patients who were older (adjusted odds ratio [aOR], 0.97 per year [95% confidence interval {CI}, .96-.98]), previously hospitalized (aOR, 0.36 [95% CI, .24-.54]), or had central lines (aOR, 0.44 [95% CI, .27-.74]), and associated with USA300 in people who inject drugs (aOR, 4.58 [95% CI, 1.16-17.95]).
Conclusions: Most of the decline in MRSA BSIs was from decreases in USA100 BSI incidence. Prevention of USA300 MRSA BSIs in the community will be needed to further reduce burden from MRSA BSIs.
Keywords: MRSA; bloodstream infections; epidemiology; infection control; strains.
Published by Oxford University Press for the Infectious Diseases Society of America 2019.
Conflict of interest statement
Figures
Similar articles
-
Evolving Epidemiology of Staphylococcus aureus Bacteremia.Infect Control Hosp Epidemiol. 2015 Dec;36(12):1417-22. doi: 10.1017/ice.2015.213. Epub 2015 Sep 16. Infect Control Hosp Epidemiol. 2015. PMID: 26372679
-
Emergence of community-associated methicillin-resistant Staphylococcus aureus strains as a cause of healthcare-associated bloodstream infections in Korea.Infect Control Hosp Epidemiol. 2009 Feb;30(2):146-55. doi: 10.1086/593953. Infect Control Hosp Epidemiol. 2009. PMID: 19128184
-
Continued emergence of USA300 methicillin-resistant Staphylococcus aureus in the United States: results from a nationwide surveillance study.Infect Control Hosp Epidemiol. 2014 Mar;35(3):285-92. doi: 10.1086/675283. Epub 2014 Jan 29. Infect Control Hosp Epidemiol. 2014. PMID: 24521595
-
Methicillin-resistant Staphylococcus aureus (MRSA): burden of disease and control challenges in Europe.Euro Surveill. 2010 Oct 14;15(41):19688. doi: 10.2807/ese.15.41.19688-en. Euro Surveill. 2010. PMID: 20961515 Review.
-
Global epidemiology of community-associated methicillin resistant Staphylococcus aureus (CA-MRSA).Curr Opin Microbiol. 2012 Oct;15(5):588-95. doi: 10.1016/j.mib.2012.08.003. Epub 2012 Oct 5. Curr Opin Microbiol. 2012. PMID: 23044073 Review.
Cited by
-
Contemporary Clinical Isolates of Staphylococcus aureus from Pediatric Osteomyelitis Patients Display Unique Characteristics in a Mouse Model of Hematogenous Osteomyelitis.Infect Immun. 2021 Sep 16;89(10):e0018021. doi: 10.1128/IAI.00180-21. Epub 2021 Jun 7. Infect Immun. 2021. PMID: 34097469 Free PMC article.
-
Bacteriological Profile and Antimicrobial Susceptibility Patterns of Gram-Negative Bloodstream Infection and Risk Factors Associated with Mortality and Drug Resistance: A Retrospective Study from Shanxi, China.Infect Drug Resist. 2022 Jul 6;15:3561-3578. doi: 10.2147/IDR.S370326. eCollection 2022. Infect Drug Resist. 2022. PMID: 35833010 Free PMC article.
-
Changes in the Genotypic Characteristics of Community-Acquired Methicillin-Resistant Staphylococcus aureus Collected in 244 Medical Facilities in Japan between 2010 and 2018: a Nationwide Surveillance.Microbiol Spectr. 2022 Aug 31;10(4):e0227221. doi: 10.1128/spectrum.02272-21. Epub 2022 Jun 27. Microbiol Spectr. 2022. PMID: 35758725 Free PMC article.
-
Investigation of Hospital-Onset Methicillin-Resistant Staphylococcus aureus Bloodstream Infections at Eight High Burden Acute Care Facilities in the United States, 2016.J Hosp Infect. 2020 Apr 10:S0195-6701(20)30182-1. doi: 10.1016/j.jhin.2020.04.007. Online ahead of print. J Hosp Infect. 2020. PMID: 32283173 Free PMC article.
-
A Sequalae of Lineage Divergence in Staphylococcus aureus from Community-Acquired Patterns in Youth to Hospital-Associated Profiles in Seniors Implied Age-Specific Host-Selection from a Common Ancestor.Diagnostics (Basel). 2023 Feb 21;13(5):819. doi: 10.3390/diagnostics13050819. Diagnostics (Basel). 2023. PMID: 36899963 Free PMC article.
References
-
- Fridkin SK, Hageman JC, Morrison M, et al. Methicillin-resistant Staphylococcus aureus disease in three communities. N Engl J Med 2005; 352:1436–44. - PubMed
-
- Herold BC, Immergluck LC, Maranan MC, et al. Community-acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA 1998; 279:593–8. - PubMed
-
- Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med 2006; 355:666–74. - PubMed
-
- Naimi TS, LeDell KH, Como-Sabetti K, et al. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA 2003; 290:2976–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
