

Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation response to PEEP: a systematic review and meta-analysis
- PMID: 30447683
- PMCID: PMC6240288
- DOI: 10.1186/s12871-018-0631-4
Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation response to PEEP: a systematic review and meta-analysis
Abstract
Background: Mortality in patients with acute respiratory distress syndrome (ARDS) remains high. These patients require mechanical ventilation strategies that include high positive end-expiratory pressure (PEEP). It remains controversial whether high PEEP can improve outcomes for ARDS patients, especially patients who show improvement in oxygenation in response to PEEP. In this meta-analysis, we aimed to evaluate the effects of high PEEP on ARDS patients.
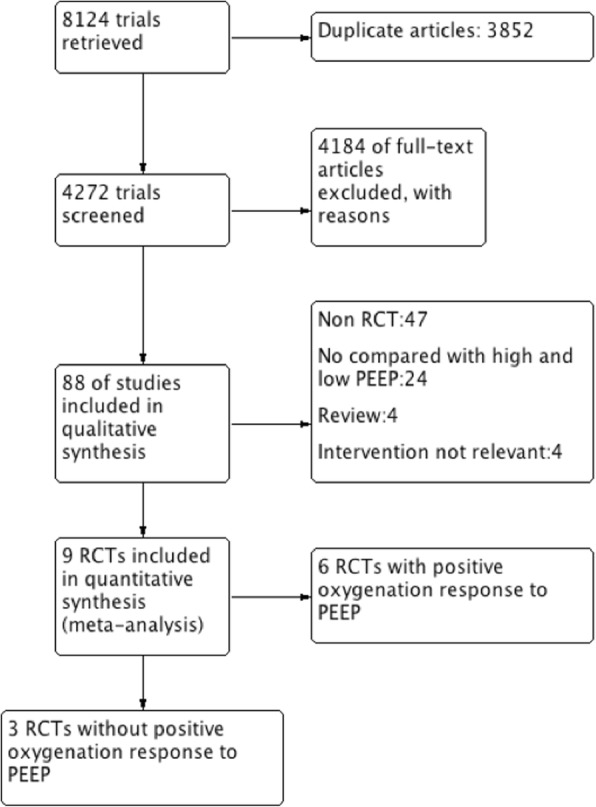
Methods: We electronically searched randomized controlled trials (RCTs) reported in the MEDLINE, CENTRAL, EMBASE, CINAHL and Web of Science databases from January 1990 to December 2017. Meta-analyses of the effects of PEEP on survival in adults with ARDS were conducted using the methods recommended by the Cochrane Collaboration.
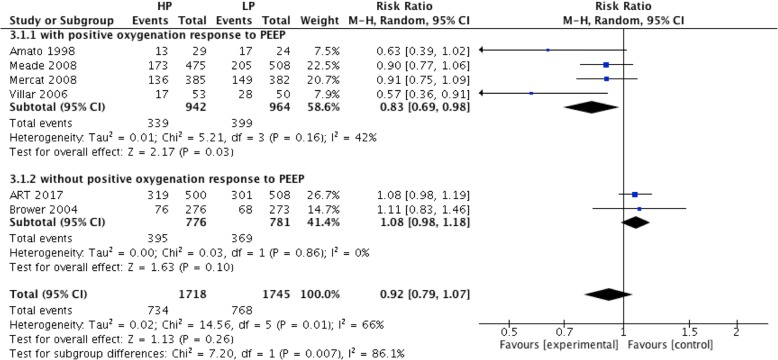
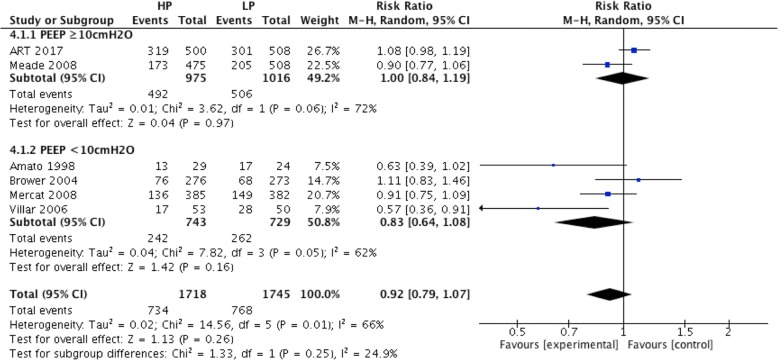
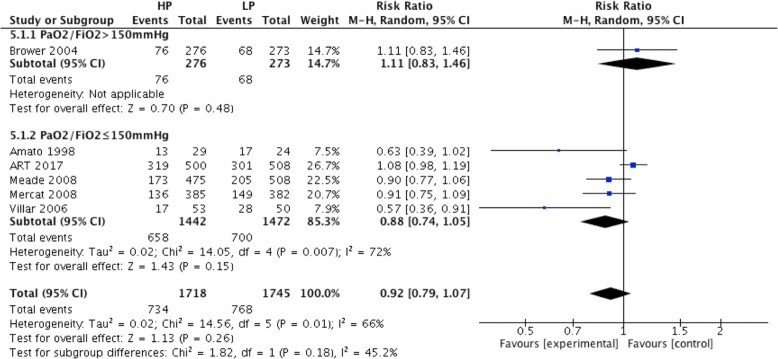
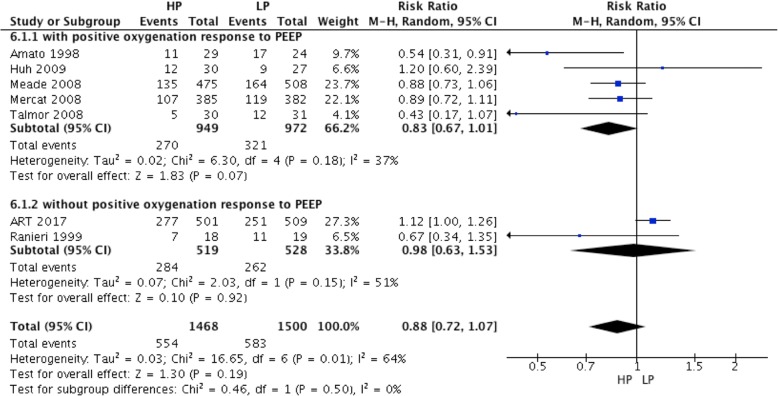
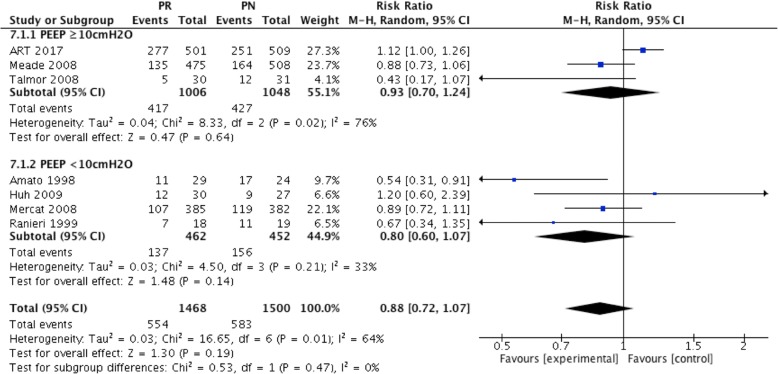
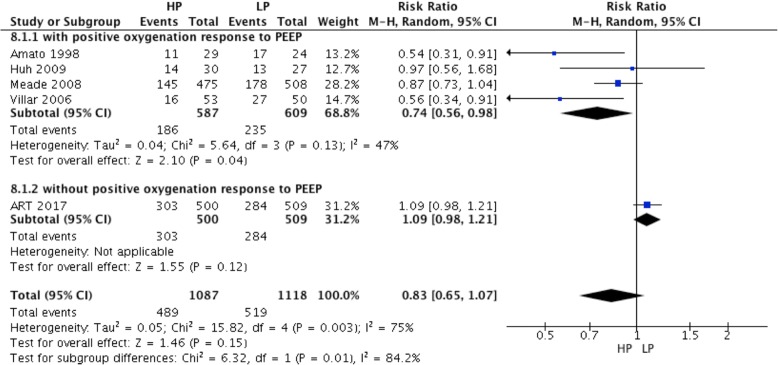
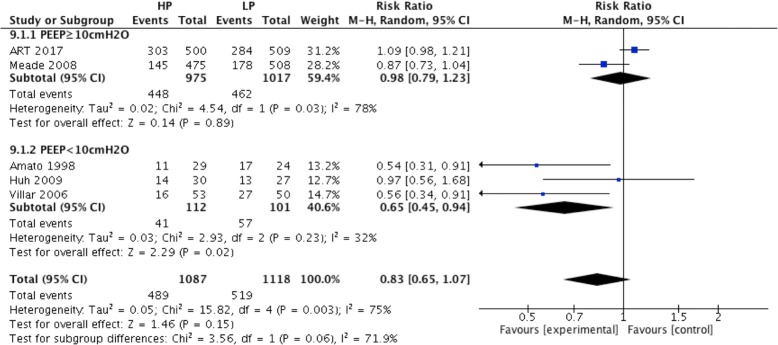
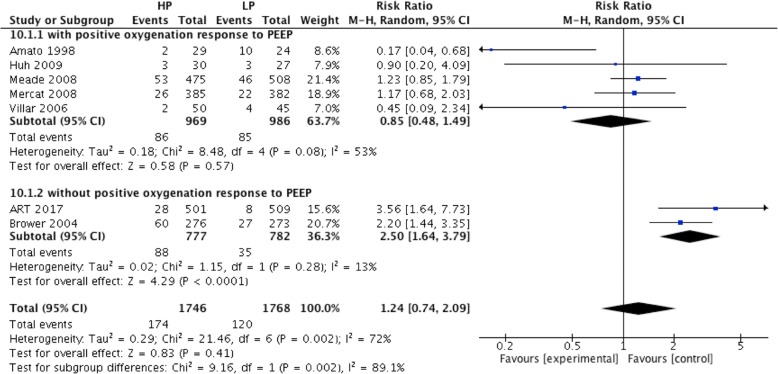
Results: A total of 3612 patients from nine randomized controlled trials (RCTs) were included. There were 1794 and 1818 patients in the high and low PEEP groups, respectively. Hospital mortality showed no significant difference between the high and low PEEP groups (RR = 0.92; 95% CI, 0.79 to 1.07; P = 0.26). Similar results were found for 28-d mortality (RR = 0.88; 95% CI, 0.72 to 1.07; P = 0.19) and ICU mortality (RR = 0.83; 95% CI, 0.65 to 1.07; P = 0.15). The risk of clinically objectified barotrauma was not significantly different between the high and low PEEP groups (RR = 1.24; 95% CI, 0.74 to 2.09, P = 0.41). In the subgroup of ARDS patients who responded to increased PEEP by improved oxygenation (from 6 RCTs), high PEEP significantly reduced hospital mortality (RR = 0.83; 95% CI 0.69 to 0.98; P = 0.03), ICU mortality (RR = 0.74; 95% CI, 0.56 to 0.98; P = 0.04),but the 28-d mortality was not decreased(RR = 0.83; 95% CI, 0.67 to 1.01; P = 0.07). For ARDS patients in the low PEEP group who received a PEEP level lower than 10 cmH2O (from 6 RCTs), ICU mortality was lower in the high PEEP group than the low PEEP group (RR = 0.65; 95% CI, 0.45 to 0.94; P = 0.02).
Conclusions: For ARDS patients who responded to increased PEEP by improved oxygenation, high PEEP could reduce hospital mortality, ICU mortality and 28-d mortality. High PEEP does not increase the risk of clinically objectified barotrauma.
Keywords: ARDS; Barotrauma; Meta; Mortality; PEEP.
Conflict of interest statement
Ethics approval and consent to participate
Not available.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis.JAMA. 2010 Mar 3;303(9):865-73. doi: 10.1001/jama.2010.218. JAMA. 2010. PMID: 20197533 Review.
-
High versus low positive end-expiratory pressure (PEEP) levels for mechanically ventilated adult patients with acute lung injury and acute respiratory distress syndrome.Cochrane Database Syst Rev. 2021 Mar 30;3(3):CD009098. doi: 10.1002/14651858.CD009098.pub3. Cochrane Database Syst Rev. 2021. PMID: 33784416 Free PMC article.
-
High versus low positive end-expiratory pressure (PEEP) levels for mechanically ventilated adult patients with acute lung injury and acute respiratory distress syndrome.Cochrane Database Syst Rev. 2013 Jun 6;2013(6):CD009098. doi: 10.1002/14651858.CD009098.pub2. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2021 Mar 30;3:CD009098. doi: 10.1002/14651858.CD009098.pub3. PMID: 23740697 Free PMC article. Updated. Review.
-
Higher PEEP versus Lower PEEP Strategies for Patients with Acute Respiratory Distress Syndrome. A Systematic Review and Meta-Analysis.Ann Am Thorac Soc. 2017 Oct;14(Supplement_4):S297-S303. doi: 10.1513/AnnalsATS.201704-338OT. Ann Am Thorac Soc. 2017. PMID: 29043834 Review.
-
Low Tidal Volume versus Non-Volume-Limited Strategies for Patients with Acute Respiratory Distress Syndrome. A Systematic Review and Meta-Analysis.Ann Am Thorac Soc. 2017 Oct;14(Supplement_4):S271-S279. doi: 10.1513/AnnalsATS.201704-337OT. Ann Am Thorac Soc. 2017. PMID: 28846440 Review.
Cited by
-
Reactive Oxygen Species and Strategies for Antioxidant Intervention in Acute Respiratory Distress Syndrome.Antioxidants (Basel). 2023 Nov 18;12(11):2016. doi: 10.3390/antiox12112016. Antioxidants (Basel). 2023. PMID: 38001869 Free PMC article. Review.
-
Efficacy of Higher Positive End-Expiratory Pressure Ventilation Strategy in Patients With Acute Respiratory Distress Syndrome: A Systematic Review and Meta-Analysis.Cureus. 2022 Jul 18;14(7):e26957. doi: 10.7759/cureus.26957. eCollection 2022 Jul. Cureus. 2022. PMID: 35989808 Free PMC article. Review.
-
American Association for the Surgery of Trauma/American College of Surgeons Committee on Trauma clinical protocol for management of acute respiratory distress syndrome and severe hypoxemia.J Trauma Acute Care Surg. 2023 Oct 1;95(4):592-602. doi: 10.1097/TA.0000000000004046. Epub 2023 Jun 12. J Trauma Acute Care Surg. 2023. PMID: 37314843 Free PMC article.
-
Pneumothorax rate in intubated patients with COVID-19.Acute Crit Care. 2021 Feb;36(1):81-84. doi: 10.4266/acc.2020.00689. Epub 2020 Dec 21. Acute Crit Care. 2021. PMID: 33342201 Free PMC article. No abstract available.
-
Ventilatory settings in the initial 72 h and their association with outcome in out-of-hospital cardiac arrest patients: a preplanned secondary analysis of the targeted hypothermia versus targeted normothermia after out-of-hospital cardiac arrest (TTM2) trial.Intensive Care Med. 2022 Aug;48(8):1024-1038. doi: 10.1007/s00134-022-06756-4. Epub 2022 Jul 2. Intensive Care Med. 2022. PMID: 35780195 Free PMC article.
References
-
- Esteban Andrés, Ferguson Niall D., Meade Maureen O., Frutos-Vivar Fernando, Apezteguia Carlos, Brochard Laurent, Raymondos Konstantinos, Nin Nicolas, Hurtado Javier, Tomicic Vinko, González Marco, Elizalde José, Nightingale Peter, Abroug Fekri, Pelosi Paolo, Arabi Yaseen, Moreno Rui, Jibaja Manuel, D'Empaire Gabriel, Sandi Fredi, Matamis Dimitros, Montañez Ana María, Anzueto Antonio. Evolution of Mechanical Ventilation in Response to Clinical Research. American Journal of Respiratory and Critical Care Medicine. 2008;177(2):170–177. doi: 10.1164/rccm.200706-893OC. - DOI - PubMed
-
- Meade MO, Cook DJ, Guyatt GH, et al. Lung open ventilation study investigators. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2008;299:637–645. doi: 10.1001/jama.299.6.637. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
