

Adult leukemia survival trends in the United States by subtype: A population-based registry study of 370,994 patients diagnosed during 1995-2009
- PMID: 30343495
- PMCID: PMC6392057
- DOI: 10.1002/cncr.31674
Adult leukemia survival trends in the United States by subtype: A population-based registry study of 370,994 patients diagnosed during 1995-2009
Abstract
Background: The lifetime risk of developing leukemia in the United States is 1.5%. There are challenges in the estimation of population-based survival using registry data because treatments and prognosis vary greatly by subtype. The objective of the current study was to determine leukemia survival estimates in the United States from 1995 to 2009 according to subtype, sex, geographical area, and race.
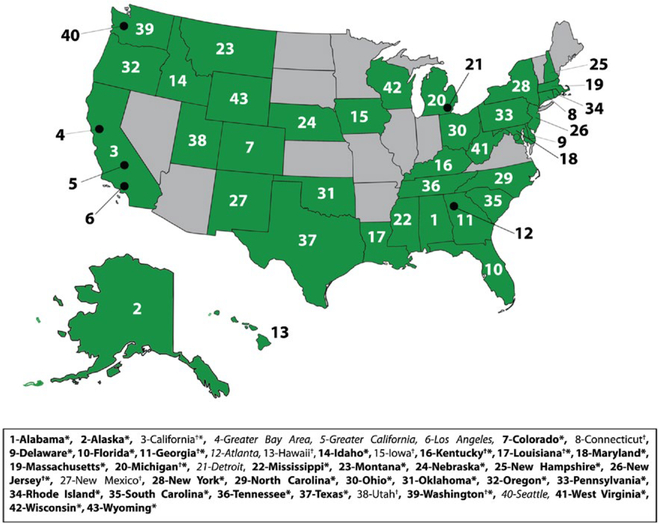
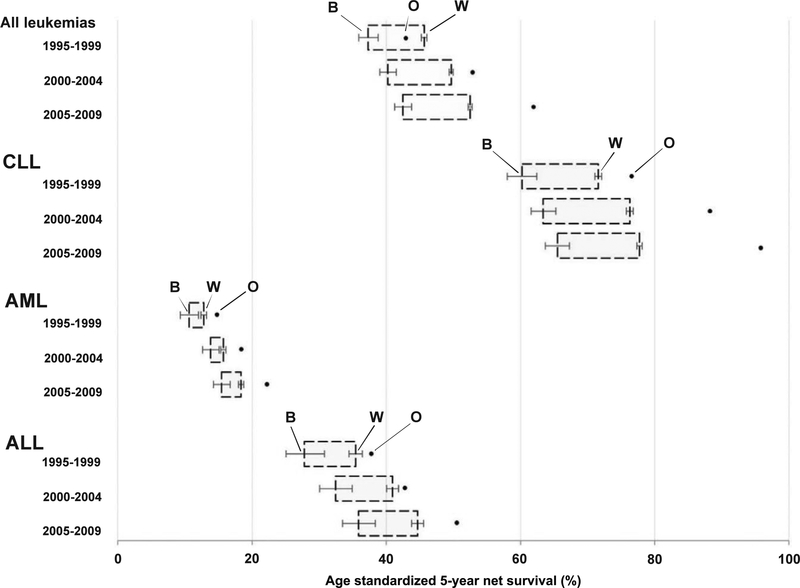
Methods: Five-year net survival was estimated using data for 370,994 patients from 43 registries in 37 states and in 6 metropolitan areas, covering approximately 81% of the adult (15-99 years) US population. Leukemia was categorized according to principal subtype (chronic lymphocytic leukemia, acute myeloid leukemia, and acute lymphocytic leukemia), and subcategorized in accordance with the HAEMACARE protocol. We analyzed age-standardized 5-year net survival by calendar period (1995-1999, 2000-2004, and 2005-2009), leukemia subtype, sex, race, and US state.
Results: The age-standardized 5-year net survival estimates increased from 45.0% for patients diagnosed during 1995-1999 to 49.0% for those diagnosed during 2000-2004 and 52.0% for those diagnosed during 2005-2009. For patients diagnosed during 2005-2009, 5-year survival was 18.2% (95% confidence interval [95% CI], 17.8%-18.6%) for acute myeloid leukemia, 44.0% (95% CI, 43.2%-44.8%) for acute lymphocytic leukemia, and 77.3% (95% CI, 76.9%-77.7%) for chronic lymphocytic leukemia. For nearly all leukemia subtypes, survival declined in successive age groups above 45 to 54 years. Men were found to have slightly lower survival than women; however, this discrepancy was noted to have fallen in successive calendar periods. Net survival was substantially higher in white than black patients in all calendar periods. There were large differences in survival noted between states and metropolitan areas.
Conclusions: Survival from leukemia in US adults improved during 1995-2009. Some geographical differences in survival may be related to access to care. We found disparities in survival by sex and between black and white patients.
Keywords: Epidemiology; National Program of Cancer Registries; Surveillance; United States; and End Results (SEER); cancer; cancer registries; leukemia; population-based survival.
© 2018 American Cancer Society.
Conflict of interest statement
Additional supporting information may be found online in the Supporting Information section at the end of the article.
CONFLICT OF INTEREST DISCLOSURES
The authors made no disclosures.
Figures
Similar articles
-
Racial disparities in the survival of American children, adolescents, and young adults with acute lymphoblastic leukemia, acute myelogenous leukemia, and Hodgkin lymphoma.Cancer. 2016 Sep 1;122(17):2723-30. doi: 10.1002/cncr.30089. Epub 2016 Jun 10. Cancer. 2016. PMID: 27286322 Free PMC article.
-
Survival among children diagnosed with acute lymphoblastic leukemia in the United States, by race and age, 2001 to 2009: Findings from the CONCORD-2 study.Cancer. 2017 Dec 15;123 Suppl 24(Suppl 24):5178-5189. doi: 10.1002/cncr.30899. Cancer. 2017. PMID: 29205314 Free PMC article.
-
Trends in leukemia incidence and survival in the United States (1973-1998).Cancer. 2003 May 1;97(9):2229-35. doi: 10.1002/cncr.11316. Cancer. 2003. PMID: 12712476
-
Racial differences in the presentation and outcomes of chronic lymphocytic leukemia and variants in the United States.Clin Lymphoma Myeloma Leuk. 2011 Dec;11(6):498-506. doi: 10.1016/j.clml.2011.07.002. Epub 2011 Sep 1. Clin Lymphoma Myeloma Leuk. 2011. PMID: 21889433
-
[Leukemia].MMW Fortschr Med. 2013 Nov 7;155(19):48-52; quiz 53. doi: 10.1007/s15006-013-2300-3. MMW Fortschr Med. 2013. PMID: 24475671 Review. German. No abstract available.
Cited by
-
Estrogens revert neutrophil hyperplasia by inhibiting Hif1α-cMyb pathway in zebrafish myelodysplastic syndromes models.Cell Death Discov. 2022 Jul 16;8(1):323. doi: 10.1038/s41420-022-01121-2. Cell Death Discov. 2022. PMID: 35842445 Free PMC article.
-
Prognostic effect of gender on outcome of treatment for adults with acute myeloid leukaemia.Br J Haematol. 2021 Jul;194(2):309-318. doi: 10.1111/bjh.17523. Epub 2021 Jun 17. Br J Haematol. 2021. PMID: 34145576 Free PMC article.
-
Survival and predictors of mortality among acute leukemia patients on follow-up in Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia: A 5-year retrospective cohort study.Cancer Rep (Hoboken). 2023 Oct;6(10):e1890. doi: 10.1002/cnr2.1890. Epub 2023 Oct 2. Cancer Rep (Hoboken). 2023. PMID: 37783566 Free PMC article.
-
Secular trends in the incidence and survival of all leukemia types in the United States from 1975 to 2017.J Cancer. 2021 Feb 22;12(8):2326-2335. doi: 10.7150/jca.52186. eCollection 2021. J Cancer. 2021. PMID: 33758609 Free PMC article.
-
miRNA probe integrated biosensor platform using bimetallic nanostars for amplification-free multiplexed detection of circulating colorectal cancer biomarkers in clinical samples.Biosens Bioelectron. 2023 Jan 15;220:114855. doi: 10.1016/j.bios.2022.114855. Epub 2022 Oct 28. Biosens Bioelectron. 2023. PMID: 36332335 Free PMC article.
References
-
- Howlader N, Noone AM, Krapcho M, eds. In: SEER Cancer Statistics Review, 1975–2014. National Cancer Institute: Bethesda, MD; 2017.
-
- Wingo PA, Jamison PM, Hiatt RA, et al. Building the infrastructure for nationwide cancer surveillance and control–a comparison between the National Program of Cancer Registries (NPCR) and the Surveillance, Epidemiology, and End Results (SEER) Program (United States). Cancer Causes Control. 2003;14:175–193. - PubMed
-
- Coleman MP. Cancer survival: global surveillance will stimulate health policy and improve equity. Lancet. 2014;383:564–573. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
