

Recommendation-based dietary indexes and risk of colorectal cancer in the Nurses' Health Study and Health Professionals Follow-up Study
- PMID: 30289433
- PMCID: PMC6250984
- DOI: 10.1093/ajcn/nqy171
Recommendation-based dietary indexes and risk of colorectal cancer in the Nurses' Health Study and Health Professionals Follow-up Study
Abstract
Background: Many dietary indexes exist for chronic disease prevention, but the optimal dietary pattern for colorectal cancer prevention is unknown.
Objective: We sought to determine associations between adherence to various dietary indexes and incident colorectal cancer in 2 prospective cohort studies.
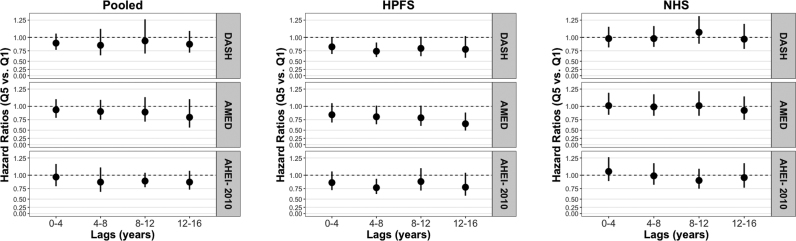
Design: We followed 78,012 women in the Nurses' Health Study and 46,695 men in the Health Professionals Follow-up Study from 1986 and 1988, respectively, until 2012. We created dietary index scores for the Dietary Approaches to Stop Hypertension (DASH) diet, Alternative Mediterranean Diet (AMED), and Alternative Healthy Eating Index-2010 (AHEI-2010) and used Cox regression to estimate HRs and 95% CIs for risk of colorectal cancer (CRC) and by anatomic subsite. We also conducted latency analyses to examine associations between diet and CRC risk during different windows of exposure. We conducted analyses in men and women separately, and subsequently pooled these results in a random-effects meta-analysis.
Results: We documented 2690 colorectal cancer cases. Pooled multivariable HRs for colorectal cancer risk comparing the highest to lowest quintile of diet scores were 0.89 (95% CI: 0.74, 1.08; P-trend = 0.10) for DASH, 0.89 (95% CI: 0.73, 1.10; P-trend = 0.31) for AMED, and 0.95 (95% CI: 0.83, 1.09; P-trend = 0.56) for AHEI-2010 (P-heterogeneity ≥ 0.07 for all). In sex-specific analyses, we observed stronger associations in men for all dietary indexes (DASH: multivariable HR = 0.81, 95% CI: 0.66, 0.98; P-trend = 0.003; AMED: multivariable HR = 0.80, 95% CI: 0.65, 0.98; P-trend = 0.02; AHEI-2010: multivariable HR = 0.88, 95% CI: 0.72, 1.07; P-trend = 0.04) than in women (multivariable HRs range from 0.98 to 1.01).
Conclusions: Adherence to the DASH, AMED, and AHEI-2010 diets was inversely associated with colorectal cancer risk in men. These diets were not associated with colorectal cancer risk in women. This observational study was registered at http://www.clinicaltrials.gov as NCT03364582.
Figures
Similar articles
-
Dietary index scores and invasive breast cancer risk among women with a family history of breast cancer.Am J Clin Nutr. 2019 May 1;109(5):1393-1401. doi: 10.1093/ajcn/nqy392. Am J Clin Nutr. 2019. PMID: 30968114 Free PMC article.
-
High-Quality Diets Associate With Reduced Risk of Colorectal Cancer: Analyses of Diet Quality Indexes in the Multiethnic Cohort.Gastroenterology. 2017 Aug;153(2):386-394.e2. doi: 10.1053/j.gastro.2017.04.004. Epub 2017 Apr 17. Gastroenterology. 2017. PMID: 28428143 Free PMC article.
-
Association of Dietary Quality With Risk of Incident Systemic Lupus Erythematosus in the Nurses' Health Study and Nurses' Health Study II.Arthritis Care Res (Hoboken). 2021 Sep;73(9):1250-1258. doi: 10.1002/acr.24443. Epub 2021 Aug 6. Arthritis Care Res (Hoboken). 2021. PMID: 32936999 Free PMC article.
-
Diet quality as assessed by the Healthy Eating Index, the Alternate Healthy Eating Index, the Dietary Approaches to Stop Hypertension score, and health outcomes: a systematic review and meta-analysis of cohort studies.J Acad Nutr Diet. 2015 May;115(5):780-800.e5. doi: 10.1016/j.jand.2014.12.009. Epub 2015 Feb 11. J Acad Nutr Diet. 2015. PMID: 25680825 Review.
-
Adherence to dietary guidelines and mortality: a report from prospective cohort studies of 134,000 Chinese adults in urban Shanghai.Am J Clin Nutr. 2014 Aug;100(2):693-700. doi: 10.3945/ajcn.113.079194. Epub 2014 Jun 18. Am J Clin Nutr. 2014. PMID: 24944055 Free PMC article. Review.
Cited by
-
Inequalities in diet quality by socio-demographic characteristics, smoking, and weight status in a large UK-based cohort using a new UK diet quality questionnaire-UKDQQ.J Nutr Sci. 2024 Oct 10;13:e59. doi: 10.1017/jns.2024.60. eCollection 2024. J Nutr Sci. 2024. PMID: 39464404 Free PMC article.
-
Adherence to the Mediterranean Diet and Colorectal Cancer Risk Among Moroccan Population: Hospital-Based Case Control Study.Asian Pac J Cancer Prev. 2024 Aug 1;25(8):2853-2860. doi: 10.31557/APJCP.2024.25.8.2853. Asian Pac J Cancer Prev. 2024. PMID: 39205583 Free PMC article.
-
Dietary Pattern and Cancer.Cancer Treat Res. 2024;191:191-216. doi: 10.1007/978-3-031-55622-7_8. Cancer Treat Res. 2024. PMID: 39133409 Review.
-
Adherence to the Mediterranean diet and its protective effects against colorectal cancer: a meta-analysis of 26 studies with 2,217,404 participants.Geroscience. 2024 Aug 1. doi: 10.1007/s11357-024-01296-9. Online ahead of print. Geroscience. 2024. PMID: 39090501
-
Association of ultra-processed food consumption with colorectal cancer risk among men and women: results from three prospective US cohort studies.BMJ. 2022 Aug 31;378:e068921. doi: 10.1136/bmj-2021-068921. BMJ. 2022. PMID: 38752573 Free PMC article.
References
-
- World Cancer Research Fund International/American Institute for Cancer Research. Continuous Update Project Report: Diet, Nutrition, Physical Activity and Colorectal Cancer. 2017.
-
- Hu FB. Dietary pattern analysis: a new direction in nutritional epidemiology. Curr Opin Lipidol. 2002;13(1):3–9. - PubMed
-
- Bamia C, Lagiou P, Buckland G, Grioni S, Agnoli C, Taylor AJ, Dahm CC, Overvad K, Olsen A, Tjonneland A et al. .. Mediterranean diet and colorectal cancer risk: results from a European cohort. Eur J Epidemiol. 2013;28(4):317–28. - PubMed
