

Addition of a polygenic risk score, mammographic density, and endogenous hormones to existing breast cancer risk prediction models: A nested case-control study
- PMID: 30180161
- PMCID: PMC6122802
- DOI: 10.1371/journal.pmed.1002644
Addition of a polygenic risk score, mammographic density, and endogenous hormones to existing breast cancer risk prediction models: A nested case-control study
Abstract
Background: No prior study to our knowledge has examined the joint contribution of a polygenic risk score (PRS), mammographic density (MD), and postmenopausal endogenous hormone levels-all well-confirmed risk factors for invasive breast cancer-to existing breast cancer risk prediction models.
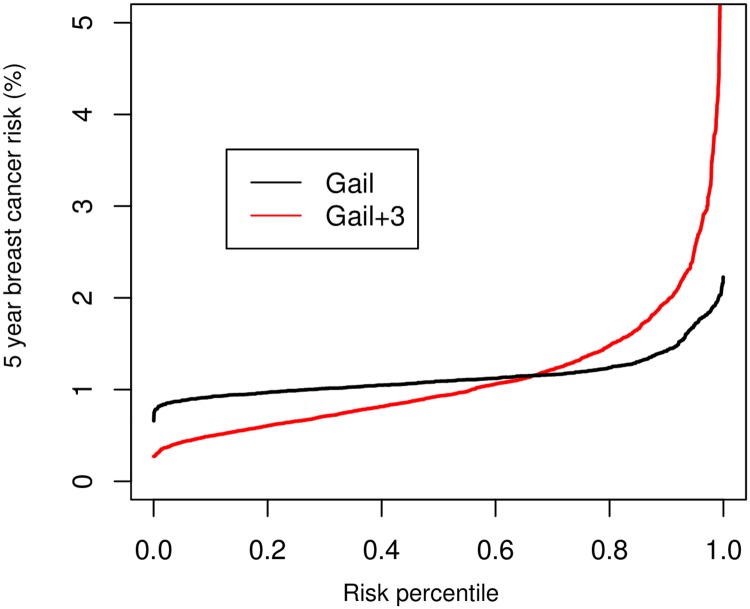
Methods and findings: We conducted a nested case-control study within the prospective Nurses' Health Study and Nurses' Health Study II including 4,006 cases and 7,874 controls ages 34-70 years up to 1 June 2010. We added a breast cancer PRS using 67 single nucleotide polymorphisms, MD, and circulating testosterone, estrone sulfate, and prolactin levels to existing risk models. We calculated area under the curve (AUC), controlling for age and stratified by menopausal status, for the 5-year absolute risk of invasive breast cancer. We estimated the population distribution of 5-year predicted risks for models with and without biomarkers. For the Gail model, the AUC improved (p-values < 0.001) from 55.9 to 64.1 (8.2 units) in premenopausal women (Gail + PRS + MD), from 55.5 to 66.0 (10.5 units) in postmenopausal women not using hormone therapy (HT) (Gail + PRS + MD + all hormones), and from 58.0 to 64.9 (6.9 units) in postmenopausal women using HT (Gail + PRS + MD + prolactin). For the Rosner-Colditz model, the corresponding AUCs improved (p-values < 0.001) by 5.7, 6.2, and 6.5 units. For estrogen-receptor-positive tumors, among postmenopausal women not using HT, the AUCs improved (p-values < 0.001) by 14.3 units for the Gail model and 7.3 units for the Rosner-Colditz model. Additionally, the percentage of 50-year-old women predicted to be at more than twice 5-year average risk (≥2.27%) was 0.2% for the Gail model alone and 6.6% for the Gail + PRS + MD + all hormones model. Limitations of our study included the limited racial/ethnic diversity of our cohort, and that general population exposure distributions were unavailable for some risk factors.
Conclusions: In this study, the addition of PRS, MD, and endogenous hormones substantially improved existing breast cancer risk prediction models. Further studies will be needed to confirm these findings and to determine whether improved risk prediction models have practical value in identifying women at higher risk who would most benefit from chemoprevention, screening, and other risk-reducing strategies.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Inclusion of endogenous hormone levels in risk prediction models of postmenopausal breast cancer.J Clin Oncol. 2014 Oct 1;32(28):3111-7. doi: 10.1200/JCO.2014.56.1068. Epub 2014 Aug 18. J Clin Oncol. 2014. PMID: 25135988 Free PMC article.
-
Inclusion of Endogenous Plasma Dehydroepiandrosterone Sulfate and Mammographic Density in Risk Prediction Models for Breast Cancer.Cancer Epidemiol Biomarkers Prev. 2020 Mar;29(3):574-581. doi: 10.1158/1055-9965.EPI-19-1120. Epub 2020 Jan 16. Cancer Epidemiol Biomarkers Prev. 2020. PMID: 31948996
-
Added Value of Serum Hormone Measurements in Risk Prediction Models for Breast Cancer for Women Not Using Exogenous Hormones: Results from the EPIC Cohort.Clin Cancer Res. 2017 Aug 1;23(15):4181-4189. doi: 10.1158/1078-0432.CCR-16-3011. Epub 2017 Feb 28. Clin Cancer Res. 2017. PMID: 28246273
-
Improvement in risk prediction, early detection and prevention of breast cancer in the NHS Breast Screening Programme and family history clinics: a dual cohort study.Southampton (UK): NIHR Journals Library; 2016 Aug. Southampton (UK): NIHR Journals Library; 2016 Aug. PMID: 27559559 Free Books & Documents. Review.
-
Relationship between estrogen levels, use of hormone replacement therapy, and breast cancer.J Natl Cancer Inst. 1998 Jun 3;90(11):814-23. doi: 10.1093/jnci/90.11.814. J Natl Cancer Inst. 1998. PMID: 9625169 Review.
Cited by
-
Cancer Progress and Priorities: Breast Cancer.Cancer Epidemiol Biomarkers Prev. 2021 May;30(5):822-844. doi: 10.1158/1055-9965.EPI-20-1193. Cancer Epidemiol Biomarkers Prev. 2021. PMID: 33947744 Free PMC article. Review. No abstract available.
-
Incorporating Polygenic Risk Scores and Nongenetic Risk Factors for Breast Cancer Risk Prediction Among Asian Women.JAMA Netw Open. 2022 Mar 1;5(3):e2149030. doi: 10.1001/jamanetworkopen.2021.49030. JAMA Netw Open. 2022. PMID: 35311964 Free PMC article.
-
Of Screening, Stratification, and Scores.J Pers Med. 2021 Jul 28;11(8):736. doi: 10.3390/jpm11080736. J Pers Med. 2021. PMID: 34442379 Free PMC article. Review.
-
Endogenous hormones and risk of invasive breast cancer in pre- and post-menopausal women: findings from the UK Biobank.Br J Cancer. 2021 Jul;125(1):126-134. doi: 10.1038/s41416-021-01392-z. Epub 2021 Apr 16. Br J Cancer. 2021. PMID: 33864017 Free PMC article.
-
Deep Learning Image Analysis of Benign Breast Disease to Identify Subsequent Risk of Breast Cancer.JNCI Cancer Spectr. 2021 Jan 11;5(1):pkaa119. doi: 10.1093/jncics/pkaa119. eCollection 2021 Feb. JNCI Cancer Spectr. 2021. PMID: 33644680 Free PMC article.
References
-
- Fisher B, Costantino JP, Wickerham DL, Redmond CK, Kavanah M, Cronin WM, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90(18):1371–88. - PubMed
-
- Costantino JP, Gail MH, Pee D, Anderson S, Redmond CK, Benichou J, et al. Validation studies for models projecting the risk of invasive and total breast cancer incidence. J Natl Cancer Inst. 1999;91(18):1541–8. - PubMed
-
- Gail MH, Brinton LA, Byar DP, Corle DK, Green SB, Schairer C, et al. Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. J Natl Cancer Inst. 1989;81(24):1879–86. - PubMed
-
- Colditz GA, Rosner B. Cumulative risk of breast cancer to age 70 years according to risk factor status: data from the Nurses’ Health Study. Am J Epidemiol. 2000;152(10):950–64. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
