

Different roles of myocardial ROCK1 and ROCK2 in cardiac dysfunction and postcapillary pulmonary hypertension in mice
- PMID: 29987023
- PMCID: PMC6064988
- DOI: 10.1073/pnas.1721298115
Different roles of myocardial ROCK1 and ROCK2 in cardiac dysfunction and postcapillary pulmonary hypertension in mice
Abstract
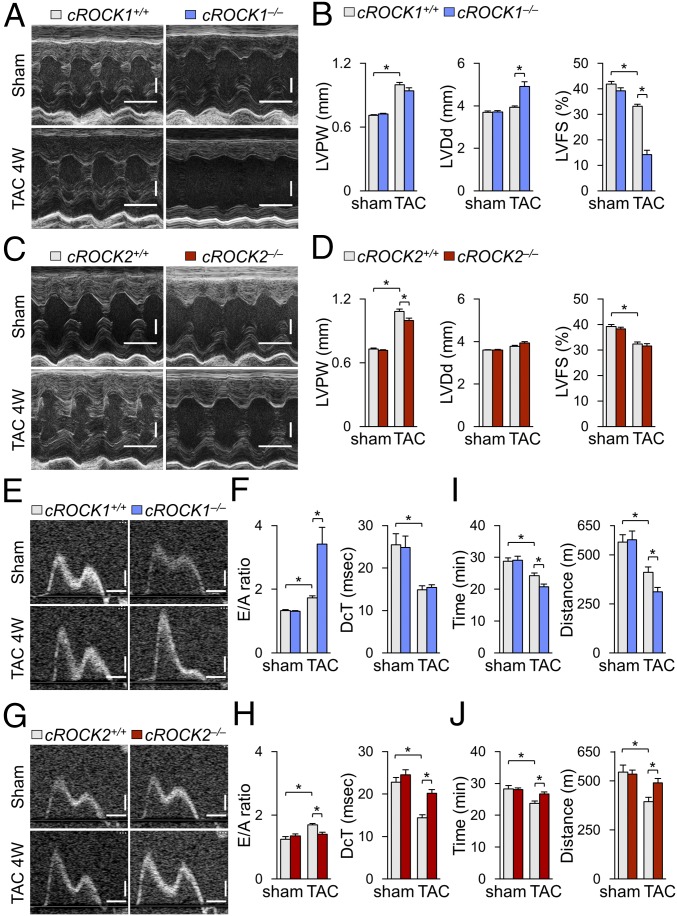
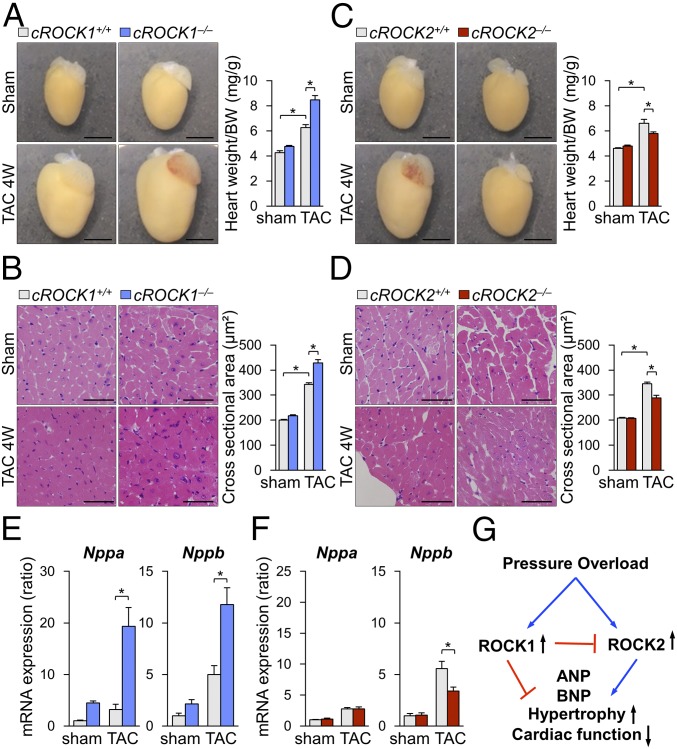
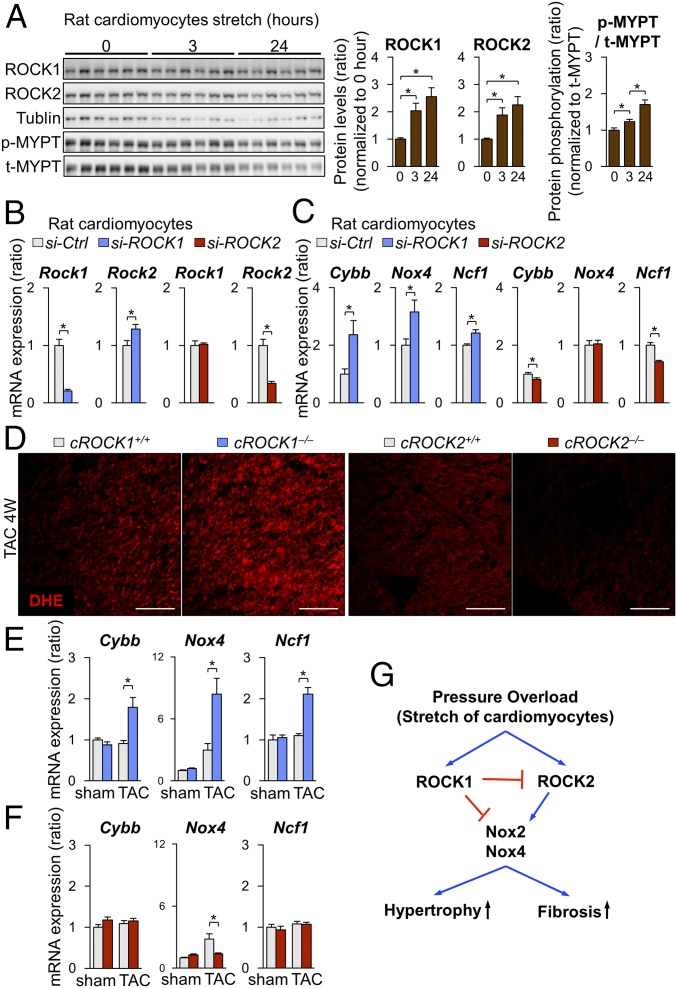
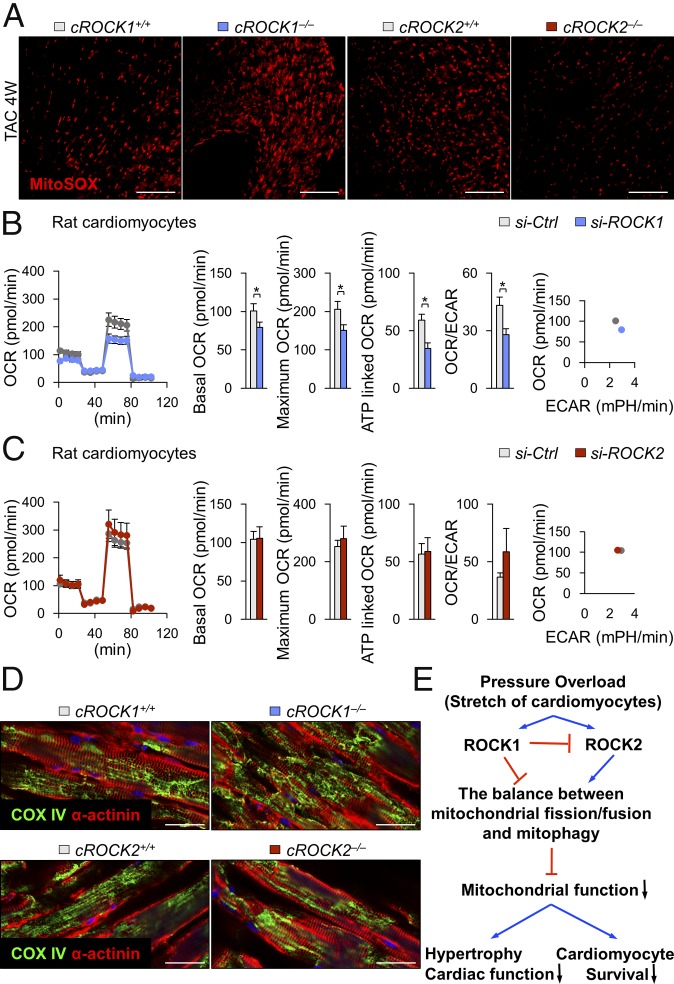
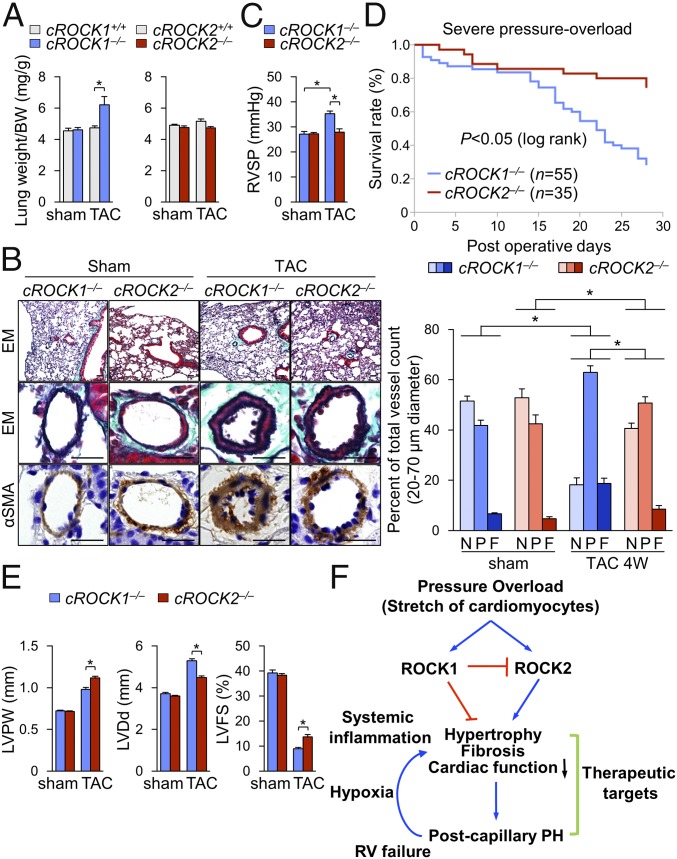
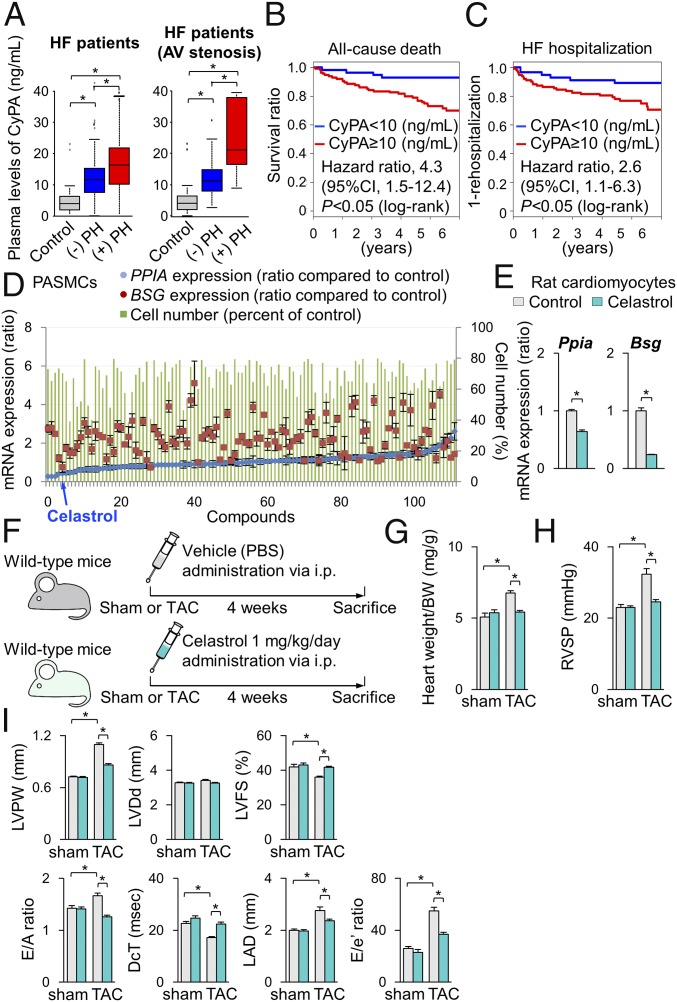
Although postcapillary pulmonary hypertension (PH) is an important prognostic factor for patients with heart failure (HF), its pathogenesis remains to be fully elucidated. To elucidate the different roles of Rho-kinase isoforms, ROCK1 and ROCK2, in cardiomyocytes in response to chronic pressure overload, we performed transverse aortic constriction (TAC) in cardiac-specific ROCK1-deficient (cROCK1-/-) and ROCK2-deficient (cROCK2-/-) mice. Cardiomyocyte-specific ROCK1 deficiency promoted pressure-overload-induced cardiac dysfunction and postcapillary PH, whereas cardiomyocyte-specific ROCK2 deficiency showed opposite results. Histological analysis showed that pressure-overload-induced cardiac hypertrophy and fibrosis were enhanced in cROCK1-/- mice compared with controls, whereas cardiac hypertrophy was attenuated in cROCK2-/- mice after TAC. Consistently, the levels of oxidative stress were up-regulated in cROCK1-/- hearts and down-regulated in cROCK2-/- hearts compared with controls after TAC. Furthermore, cyclophilin A (CyPA) and basigin (Bsg), both of which augment oxidative stress, enhanced cardiac dysfunction and postcapillary PH in cROCK1-/- mice, whereas their expressions were significantly lower in cROCK2-/- mice. In clinical studies, plasma levels of CyPA were significantly increased in HF patients and were higher in patients with postcapillary PH compared with those without it. Finally, high-throughput screening demonstrated that celastrol, an antioxidant and antiinflammatory agent, reduced the expressions of CyPA and Bsg in the heart and the lung, ameliorating cardiac dysfunction and postcapillary PH induced by TAC. Thus, by differentially affecting CyPA and Bsg expressions, ROCK1 protects and ROCK2 jeopardizes the heart from pressure-overload HF with postcapillary PH, for which celastrol may be a promising agent.
Keywords: Rho-kinase; heart failure; oxidative stress.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Identification of Celastrol as a Novel Therapeutic Agent for Pulmonary Arterial Hypertension and Right Ventricular Failure Through Suppression of Bsg (Basigin)/CyPA (Cyclophilin A).Arterioscler Thromb Vasc Biol. 2021 Mar;41(3):1205-1217. doi: 10.1161/ATVBAHA.120.315731. Epub 2021 Jan 21. Arterioscler Thromb Vasc Biol. 2021. PMID: 33472404
-
Basigin Promotes Cardiac Fibrosis and Failure in Response to Chronic Pressure Overload in Mice.Arterioscler Thromb Vasc Biol. 2016 Apr;36(4):636-46. doi: 10.1161/ATVBAHA.115.306686. Epub 2016 Feb 25. Arterioscler Thromb Vasc Biol. 2016. PMID: 26916734
-
Basigin mediates pulmonary hypertension by promoting inflammation and vascular smooth muscle cell proliferation.Circ Res. 2014 Sep 26;115(8):738-50. doi: 10.1161/CIRCRESAHA.115.304563. Epub 2014 Aug 22. Circ Res. 2014. PMID: 25149188
-
Rho Kinases and Cardiac Remodeling.Circ J. 2016 Jun 24;80(7):1491-8. doi: 10.1253/circj.CJ-16-0433. Epub 2016 Jun 1. Circ J. 2016. PMID: 27251065 Free PMC article. Review.
-
Development of Novel Therapies for Cardiovascular Diseases by Clinical Application of Basic Research.Circ J. 2017 Oct 25;81(11):1557-1563. doi: 10.1253/circj.CJ-17-1029. Epub 2017 Oct 6. Circ J. 2017. PMID: 28993547 Review.
Cited by
-
Mitochondrial connexin43 and mitochondrial KATP channels modulate triggered arrhythmias in mouse ventricular muscle.Pflugers Arch. 2023 Apr;475(4):477-488. doi: 10.1007/s00424-023-02789-w. Epub 2023 Jan 28. Pflugers Arch. 2023. PMID: 36707457
-
RhoGTPase in Vascular Disease.Cells. 2019 Jun 6;8(6):551. doi: 10.3390/cells8060551. Cells. 2019. PMID: 31174369 Free PMC article. Review.
-
Chronic Thromboembolic Pulmonary Hypertension - What Have We Learned From Large Animal Models.Front Cardiovasc Med. 2021 Apr 16;8:574360. doi: 10.3389/fcvm.2021.574360. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 33937352 Free PMC article. Review.
-
Different Aspects of Emetine's Capabilities as a Highly Potent SARS-CoV-2 Inhibitor against COVID-19.ACS Pharmacol Transl Sci. 2022 May 23;5(6):387-399. doi: 10.1021/acsptsci.2c00045. eCollection 2022 Jun 10. ACS Pharmacol Transl Sci. 2022. PMID: 35702393 Free PMC article. Review.
-
Rho Kinases in Embryonic Development and Stem Cell Research.Arch Immunol Ther Exp (Warsz). 2022 Jan 19;70(1):4. doi: 10.1007/s00005-022-00642-z. Arch Immunol Ther Exp (Warsz). 2022. PMID: 35043239 Free PMC article. Review.
References
-
- Paulus WJ, van Ballegoij JJ. Treatment of heart failure with normal ejection fraction: An inconvenient truth! J Am Coll Cardiol. 2010;55:526–537. - PubMed
-
- Holland DJ, Kumbhani DJ, Ahmed SH, Marwick TH. Effects of treatment on exercise tolerance, cardiac function, and mortality in heart failure with preserved ejection fraction. A meta-analysis. J Am Coll Cardiol. 2011;57:1676–1686. - PubMed
-
- Redfield MM. Understanding “diastolic” heart failure. N Engl J Med. 2004;350:1930–1931. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
