

The appropriate management algorithm for diabetic foot: A single-center retrospective study over 12 years
- PMID: 29979449
- PMCID: PMC6076129
- DOI: 10.1097/MD.0000000000011454
The appropriate management algorithm for diabetic foot: A single-center retrospective study over 12 years
Abstract
Background: Diabetic foot management is a challenge for reconstructive surgeons because it combines dramatically decreased circulation and chronic infection. The goal of managing this condition is to maximize viable tissue; however, unsatisfactory results, such as extremity amputation, are unavoidable in some cases. For appropriate management, thorough understanding of diabetic foot and the phased approach to its management is needed. The purpose of this study is to introduce an optimal algorithm for diabetic foot management by analyzing cases >12 years.
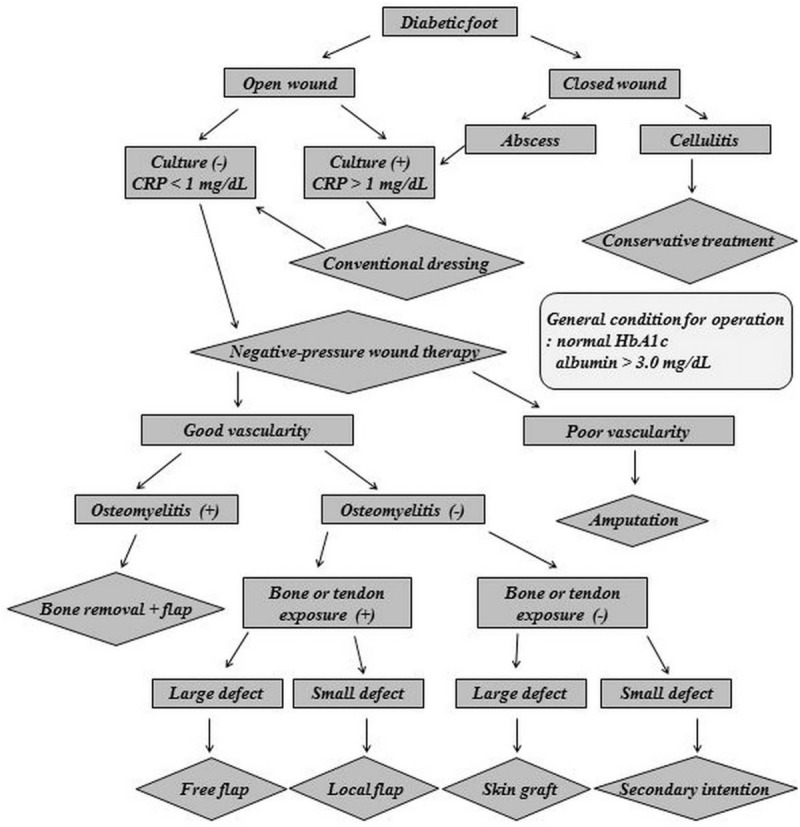
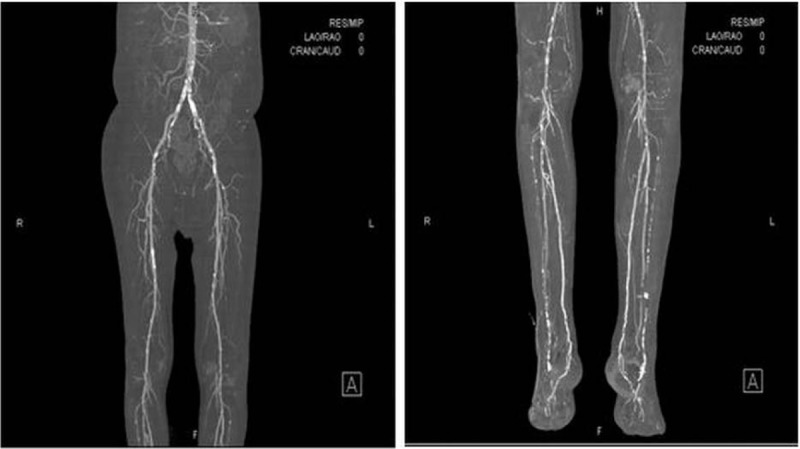
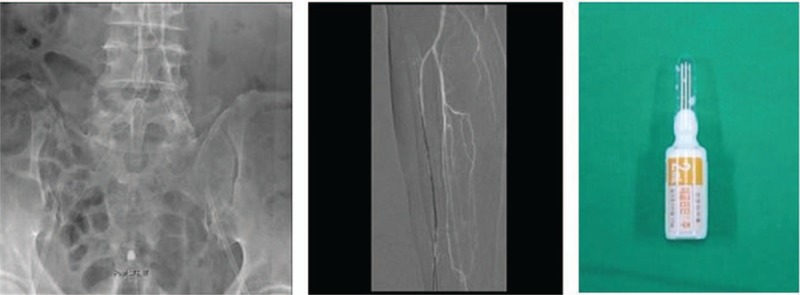
Methods: A total of 274 patients with diabetic foot at Hanyang University Guri Hospital from 2005 to 2017 were reviewed. The management process was divided into 5 steps: patient evaluation, wound preparation, improving vascularity, surgery and dressing, and rehabilitation. Patient evaluation included a microbial culture, evaluation of vascularity, and an osteomyelitis assessment. During wound preparation, debridement and negative-pressure wound therapy were performed. Vascularity was improved by radiological intervention or surgical method. Surgery and dressing were performed depending on the indications. Rehabilitation was started after complete wound healing.
Results: An infection was confirmed in 213 of 263 patients (81.0%). Of 74 cases in which a vascular study was performed, 83.8% showed arterial occlusion. When surgery was performed with complete eradication of the infection in 155 patients, the rate of revision surgery was 20.6%. The revision rate after surgery with a remnant infection of 66 patients was 40.9% (P = .0003). When surgery was performed after successful revascularization for improving blood flow of 47 patients, the rate of revision surgery was 21.3%. In contrast, the revision rate after surgery with unsuccessful or no revascularization of 174 patients was 28.2% (P = .359).
Conclusion: Diabetic foot is a debilitating disease arising from multifactorial process. As its management is complex, a comprehensive but accessible treatment algorithm is needed for successful results. For this reason, the appropriate algorithm for diabetic foot management introduced in this study is significant.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures




Similar articles
-
Outcomes after foot surgery in people with a diabetic foot ulcer and a 12-month follow-up.J Wound Care. 2017 May 2;26(5):218-227. doi: 10.12968/jowc.2017.26.5.218. J Wound Care. 2017. PMID: 28475445
-
Poorly designed research does not help clarify the role of hyperbaric oxygen in the treatment of chronic diabetic foot ulcers.Diving Hyperb Med. 2016 Sep;46(3):133-134. Diving Hyperb Med. 2016. PMID: 27723012
-
Proximal Tibial Cortex Transverse Distraction Facilitating Healing and Limb Salvage in Severe and Recalcitrant Diabetic Foot Ulcers.Clin Orthop Relat Res. 2020 Apr;478(4):836-851. doi: 10.1097/CORR.0000000000001075. Clin Orthop Relat Res. 2020. PMID: 31794478 Free PMC article.
-
Vascular evaluation and arterial reconstruction of the diabetic foot.Clin Podiatr Med Surg. 2003 Oct;20(4):689-708. doi: 10.1016/S0891-8422(03)00088-0. Clin Podiatr Med Surg. 2003. PMID: 14636033 Review.
-
Autolytic debridement of a large, necrotic, fully occluded foot ulcer using a hydrocolloid dressing in a diabetic patient.Adv Skin Wound Care. 2013 Jul;26(7):300-4. doi: 10.1097/01.ASW.0000429779.48138.c0. Adv Skin Wound Care. 2013. PMID: 23777879 Review.
Cited by
-
Species-Specific Immunoassay Aids Identification of Pathogen and Tracks Infectivity in Foot Infection.Foot Ankle Int. 2021 Mar;42(3):363-372. doi: 10.1177/1071100720965136. Epub 2020 Nov 9. Foot Ankle Int. 2021. PMID: 33161780 Free PMC article.
-
Diabetic foot and peripheral arterial disease. Single centre experience.Saudi Med J. 2021 Jan;42(1):49-55. doi: 10.15537/smj.2021.1.25640. Saudi Med J. 2021. PMID: 33399171 Free PMC article.
-
The influence of primary and subsequent limb amputation on the overall rate of limb amputation in Saskatchewan, Canada, 2006-2019: a population-based study.BMC Surg. 2021 Oct 30;21(1):385. doi: 10.1186/s12893-021-01381-2. BMC Surg. 2021. PMID: 34717614 Free PMC article.
-
Clinical, Pathological and Microbiological Evaluation of Diabetic Foot Syndrome.Medicina (Kaunas). 2020 Jul 28;56(8):380. doi: 10.3390/medicina56080380. Medicina (Kaunas). 2020. PMID: 32731610 Free PMC article.
-
Flexible electrical stimulation device with Chitosan-Vaseline® dressing accelerates wound healing in diabetes.Bioact Mater. 2020 Aug 19;6(1):230-243. doi: 10.1016/j.bioactmat.2020.08.003. eCollection 2021 Jan. Bioact Mater. 2020. PMID: 32913931 Free PMC article.
References
-
- Allen LL, Kalmar G, Driver VR. Treatment of a high-risk diabetic patient with peripheral vascular disease and osteomyelitis. Tech Vasc Interv Radiol 2016;19:96–100. - PubMed
-
- Dolan NC, Liu K, Criqui MH, et al. Peripheral artery disease, diabetes, and reduced lower extremity functioning. Diabetes Care 2002;25:113–20. - PubMed
-
- Bouton AJ, Vileikyte L, Ragnarson-Tennvall G, et al. The global burden of diabeteic foot disease. Lancet 2005;366:1719–24. - PubMed
-
- Acar E, Kacıra BK. Predictors of lower extremity amputation and reamputation in the diabetic foot. J Foot Ankle Surg 2017;56:1218–22. - PubMed
-
- Lipsky BA, Berendt AR, Deery HG, et al. Diagnosis and treatment of diabetic foot infections. Plast Reconstr Surg 2006;117:212S–38S. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
