

Longitudinal Assessment of Multidrug-Resistant Organisms in Newly Admitted Nursing Facility Patients: Implications for an Evolving Population
- PMID: 29635360
- PMCID: PMC6117444
- DOI: 10.1093/cid/ciy194
Longitudinal Assessment of Multidrug-Resistant Organisms in Newly Admitted Nursing Facility Patients: Implications for an Evolving Population
Abstract
Background: The spread of multidrug-resistant organisms (MDROs) is a global concern, and much about transmission in healthcare systems remains unknown. To reduce hospital stays, nursing facilities (NFs) have increasingly assumed care of post-acute populations. We estimate the prevalence of MDRO colonization in NF patients on enrollment and discharge to community settings, risk factors for colonization, and rates of acquiring MDROs during the stay.
Methods: We conducted a prospective, longitudinal cohort study of newly admitted patients in 6 NFs in southeast Michigan using active microbial surveillance of multiple anatomic sites sampled at enrollment, days 14 and 30, and monthly thereafter for up to 6 months.
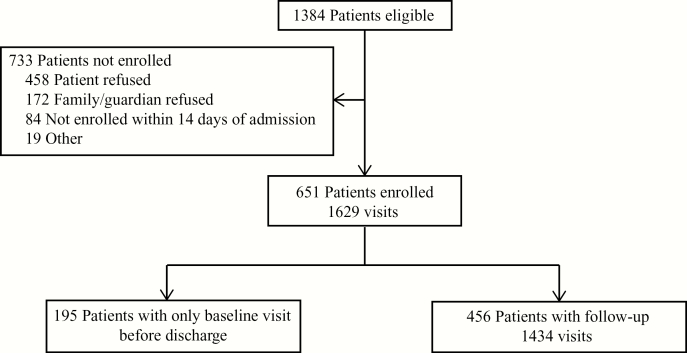
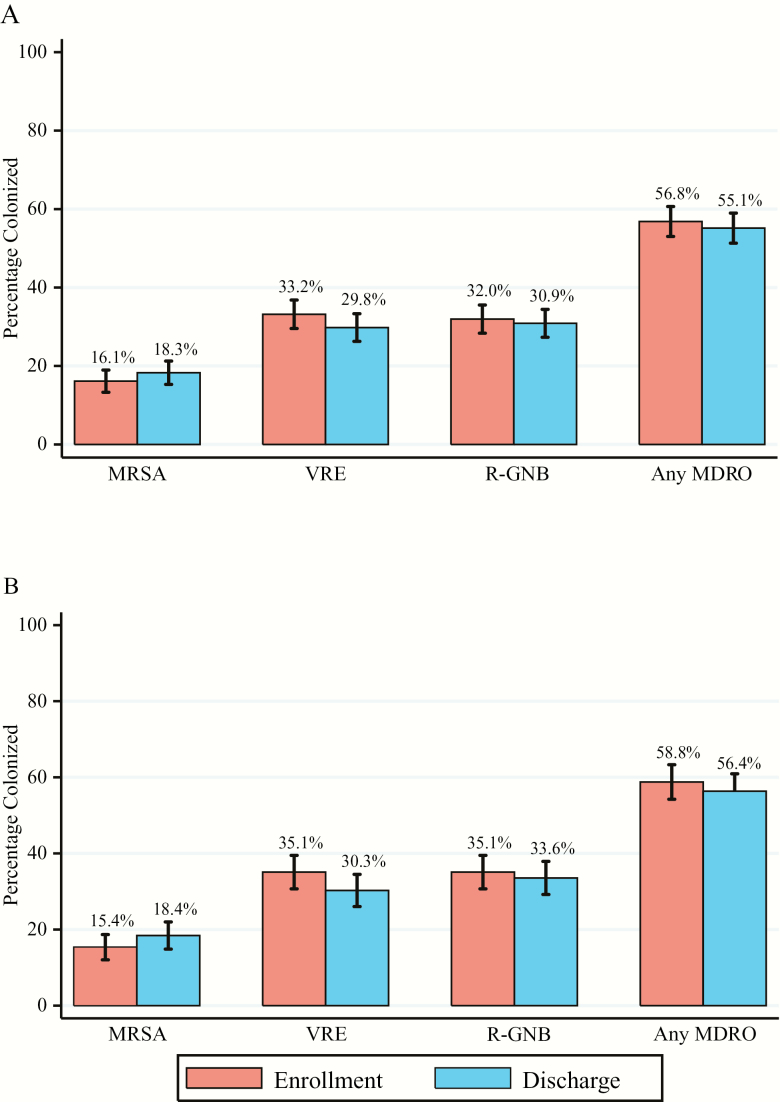
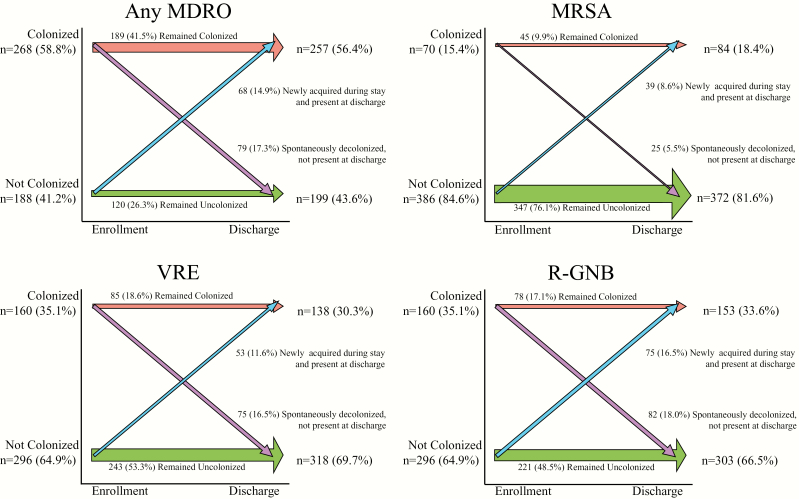
Results: We enrolled 651 patients and collected 7526 samples over 1629 visits, with an average of 29 days of follow-up per participant. Nearly all participants were admitted for post-acute care (95%). More than half (56.8%) were colonized with MDROs at enrollment: methicillin-resistant Staphylococcus aureus (MRSA), 16.1%; vancomycin-resistant enterococci (VRE), 33.2%; and resistant gram-negative bacilli (R-GNB), 32.0%. Risk factors for colonization at enrollment included prolonged hospitalization (>14 days), functional disability, antibiotic use, or device use. Rates per 1000 patient-days of acquiring a new MDRO were MRSA, 3.4; VRE, 8.2; and R-GNB, 13.6. MDRO colonization at discharge was similar to that at enrollment (56.4%): MRSA, 18.4%; VRE, 30.3%; and R-GNB, 33.6%.
Conclusions: Short-stay NF patients exhibit a high prevalence of MDROs near the time of admission, as well as at discharge, and may serve as a reservoir for spread in other healthcare settings. Future interventions to reduce MDROs should specifically target this population.
Figures
Similar articles
-
Predictors of methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci co-colonization among nursing facility patients.Am J Infect Control. 2019 Apr;47(4):415-420. doi: 10.1016/j.ajic.2018.09.026. Epub 2018 Nov 28. Am J Infect Control. 2019. PMID: 30502107 Free PMC article.
-
Clinical outcomes of intestinal transplant recipients colonized with multidrug-resistant organisms: a retrospective study.Transpl Int. 2017 Sep;30(9):924-931. doi: 10.1111/tri.12987. Epub 2017 Jul 17. Transpl Int. 2017. PMID: 28544183
-
Prevalence of multidrug-resistant organisms in nursing homes in Belgium in 2015.PLoS One. 2019 Mar 28;14(3):e0214327. doi: 10.1371/journal.pone.0214327. eCollection 2019. PLoS One. 2019. PMID: 30921364 Free PMC article.
-
[Development of antimicrobial resistance in Germany : What is the current situation?].Med Klin Intensivmed Notfmed. 2017 Apr;112(3):186-191. doi: 10.1007/s00063-017-0272-2. Epub 2017 Apr 4. Med Klin Intensivmed Notfmed. 2017. PMID: 28378152 Review. German.
-
Approaches to multidrug-resistant organism prevention and control in long-term care facilities for older people: a systematic review and meta-analysis.Antimicrob Resist Infect Control. 2022 Jan 15;11(1):7. doi: 10.1186/s13756-021-01044-0. Antimicrob Resist Infect Control. 2022. PMID: 35033198 Free PMC article. Review.
Cited by
-
Not too close! impact of roommate status on MRSA and VRE colonization and contamination in Nursing Homes.Antimicrob Resist Infect Control. 2021 Jul 5;10(1):104. doi: 10.1186/s13756-021-00972-1. Antimicrob Resist Infect Control. 2021. PMID: 34225783 Free PMC article.
-
Predictors of methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci co-colonization among nursing facility patients.Am J Infect Control. 2019 Apr;47(4):415-420. doi: 10.1016/j.ajic.2018.09.026. Epub 2018 Nov 28. Am J Infect Control. 2019. PMID: 30502107 Free PMC article.
-
Can alternative anatomical sites and environmental surveillance replace perianal screening for multidrug-resistant organisms in nursing homes?Infect Control Hosp Epidemiol. 2022 Aug;43(8):1063-1066. doi: 10.1017/ice.2021.134. Epub 2021 May 21. Infect Control Hosp Epidemiol. 2022. PMID: 34016196 Free PMC article.
-
Changing dynamics of colonization in nursing facility patients over time: Reduction in methicillin-resistant Staphylococcus aureus (MRSA) offset by increase in vancomycin-resistant Enterococcus (VRE) prevalence.Infect Control Hosp Epidemiol. 2019 Sep;40(9):1069-1070. doi: 10.1017/ice.2019.169. Epub 2019 Jun 27. Infect Control Hosp Epidemiol. 2019. PMID: 31244459 Free PMC article. No abstract available.
-
Epidemiology of resistant gram-negative bacteria in nursing homes.Infect Control Hosp Epidemiol. 2023 Sep;44(9):1423-1428. doi: 10.1017/ice.2022.225. Epub 2023 Mar 14. Infect Control Hosp Epidemiol. 2023. PMID: 36916011 Free PMC article.
References
-
- Medicare Payment Advisory Commission. Report to the Congress: Medicare payment policy 2017. Available at: http://www.medpac.gov/docs/default-source/reports/mar17_entirereport2246.... Accessed 14 November 2017.
-
- Burke RE, Juarez-Colunga E, Levy C, Prochazka AV, Coleman EA, Ginde AA. Rise of post-acute care facilities as a discharge destination of US hospitalizations. JAMA Intern Med 2015; 175:295–6. - PubMed
-
- Jenq GY, Tinetti ME. Post-acute care: who belongs where?JAMA Intern Med 2015; 175:296–7. - PubMed
-
- Weiner LM, Webb AK, Limbago B, et al. . Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2011–2014. Infect Control Hosp Epidemiol 2016; 37:1288–301. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
