

Identification of sarilumab pharmacodynamic and predictive markers in patients with inadequate response to TNF inhibition: a biomarker substudy of the phase 3 TARGET study
- PMID: 29556418
- PMCID: PMC5856917
- DOI: 10.1136/rmdopen-2017-000607
Identification of sarilumab pharmacodynamic and predictive markers in patients with inadequate response to TNF inhibition: a biomarker substudy of the phase 3 TARGET study
Abstract
Introduction: Interleukin-6 (IL-6) orchestrates formation of an inflammatory pannus, leading to joint damage in rheumatoid arthritis (RA). Sarilumab is a human monoclonal antibody blocking the IL-6Rα. In TARGET (NCT01709578), a phase 3 study in adults with moderate-to-severe RA and inadequate response or intolerance to tumour necrosis factor inhibitors, subcutaneous sarilumab 200 mg or 150 mg every 2 weeks (q2w) plus conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) significantly reduced disease activity versus placebo plus csDMARDs.
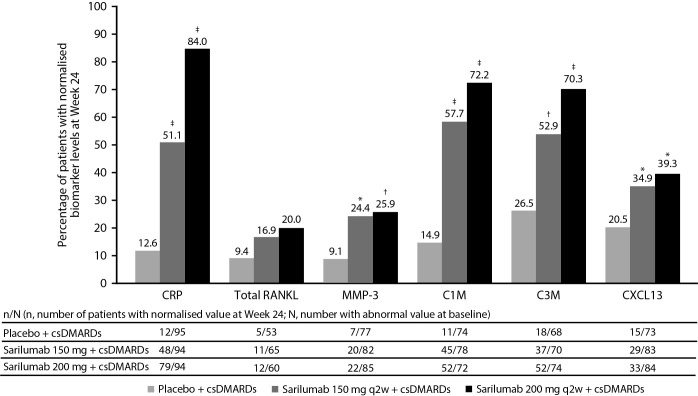
Methods: Circulating levels of biomarkers associated with synovial inflammation (matrix metalloproteinase 3 (MMP-3), collagen type I MMP-cleaved fragment (C1M), collagen type III MMP-cleaved fragment (C3M)), myeloid (soluble intercellular adhesion molecule 1 (sICAM-1), IL-8 and calprotectin) and lymphoid activation (chemokine, CXC motif, ligand 13 (CXCL13), CXCL10, B cell-activating factor) and bone remodelling (receptor activator of nuclear factor-κB ligand (RANKL), osteoprotegerin and osteocalcin) were evaluated in patients from a TARGET substudy.
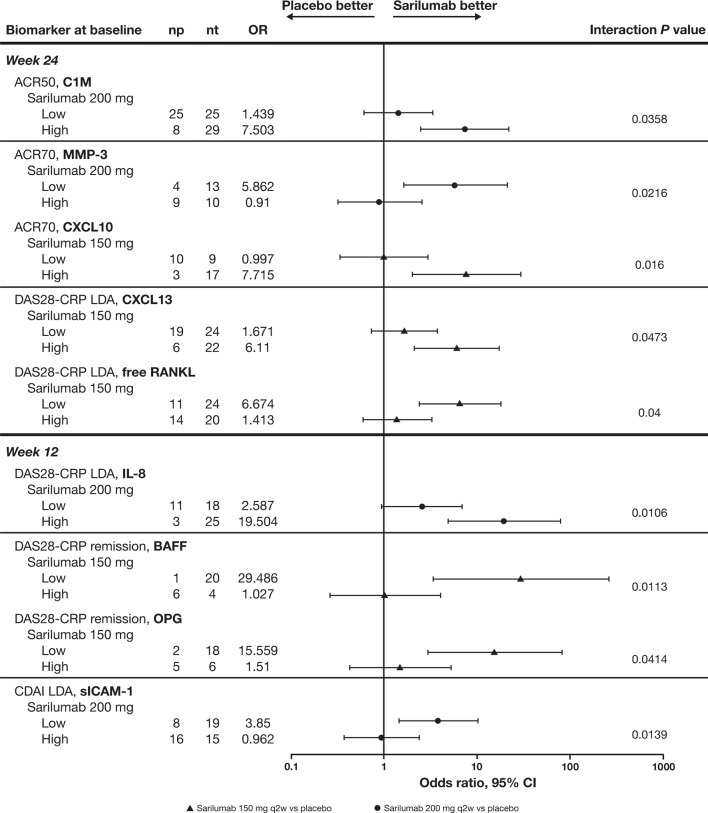
Results: Sarilumab significantly decreased C1M, C3M, CXCL13, MMP-3 and total RANKL levels at week 24 versus placebo; some markers were significantly suppressed at week 2 and normalised to levels in healthy controls. Levels of sICAM-1 were predictive of disease activity score by C-reactive protein and clinical disease activity index low disease activity (LDA) response in the sarilumab 200 mg q2w group at week 12. A trend was observed in which patients with lower sICAM-1 levels at baseline had better response compared with patients with higher sICAM-1.
Conclusions: Sarilumab plus csDMARDs decreased circulating biomarkers of synovial inflammation and bone resorption; sICAM-1 was predictive of achieving LDA with sarilumab.
Trial registration number: NCT01709578; Post-results.
Keywords: dmards (biologic); rheumatoid arthritis; treatment.
Conflict of interest statement
Competing interests: CG has received consulting fees from Roche, Merck, AbbVie, Pfizer, Bristol-Myers Squibb, Sanofi and AB2 Bio. JM, MZ and CP are employees of Sanofi R&D and may hold stock and/or stock options in the company. YL is an employee of Sanofi Genzyme and may hold stock and/or stock options in the company. NMHG and AB are employees of Regeneron Pharmaceuticals, Inc, and may hold stock and/or stock options in the company.
Figures

Similar articles
-
Sarilumab plus methotrexate suppresses circulating biomarkers of bone resorption and synovial damage in patients with rheumatoid arthritis and inadequate response to methotrexate: a biomarker study of MOBILITY.Arthritis Res Ther. 2016 Oct 6;18(1):225. doi: 10.1186/s13075-016-1132-9. Arthritis Res Ther. 2016. PMID: 27716324 Free PMC article. Clinical Trial.
-
Sarilumab and adalimumab differential effects on bone remodelling and cardiovascular risk biomarkers, and predictions of treatment outcomes.Arthritis Res Ther. 2020 Apr 7;22(1):70. doi: 10.1186/s13075-020-02163-6. Arthritis Res Ther. 2020. PMID: 32264972 Free PMC article. Clinical Trial.
-
Sarilumab, a fully human monoclonal antibody against IL-6Rα in patients with rheumatoid arthritis and an inadequate response to methotrexate: efficacy and safety results from the randomised SARIL-RA-MOBILITY Part A trial.Ann Rheum Dis. 2014 Sep;73(9):1626-34. doi: 10.1136/annrheumdis-2013-204405. Epub 2013 Dec 2. Ann Rheum Dis. 2014. PMID: 24297381 Free PMC article. Clinical Trial.
-
Sarilumab: Review of a Second IL-6 Receptor Antagonist Indicated for the Treatment of Rheumatoid Arthritis.Ann Pharmacother. 2018 Aug;52(8):780-791. doi: 10.1177/1060028018761599. Epub 2018 Feb 26. Ann Pharmacother. 2018. PMID: 29482351 Review.
-
Sarilumab: A Review in Moderate to Severe Rheumatoid Arthritis.Drugs. 2018 Jun;78(9):929-940. doi: 10.1007/s40265-018-0929-z. Drugs. 2018. PMID: 29931592 Review.
Cited by
-
A systematic literature review informing the consensus statement on efficacy and safety of pharmacological treatment with interleukin-6 pathway inhibition with biological DMARDs in immune-mediated inflammatory diseases.RMD Open. 2022 Sep;8(2):e002359. doi: 10.1136/rmdopen-2022-002359. RMD Open. 2022. PMID: 36260501 Free PMC article.
-
Toward Overcoming Treatment Failure in Rheumatoid Arthritis.Front Immunol. 2021 Dec 23;12:755844. doi: 10.3389/fimmu.2021.755844. eCollection 2021. Front Immunol. 2021. PMID: 35003068 Free PMC article. Review.
-
Predicting treatment response to IL6R blockers in rheumatoid arthritis.Rheumatology (Oxford). 2020 Dec 1;59(12):3603-3610. doi: 10.1093/rheumatology/keaa529. Rheumatology (Oxford). 2020. PMID: 32864695 Free PMC article. Review.
-
Tailored therapeutic decision of rheumatoid arthritis using proteomic strategies: how to start and when to stop?Clin Proteomics. 2023 Jun 10;20(1):22. doi: 10.1186/s12014-023-09411-2. Clin Proteomics. 2023. PMID: 37301840 Free PMC article. Review.
-
Molecular and Cellular Mechanisms of Arthritis in Children and Adults: New Perspectives on Applied Photobiomodulation.Int J Mol Sci. 2020 Sep 8;21(18):6565. doi: 10.3390/ijms21186565. Int J Mol Sci. 2020. PMID: 32911717 Free PMC article. Review.
References
-
- Desgeorges A, Gabay C, Silacci P, et al. . Concentrations and origins of soluble interleukin 6 receptor-alpha in serum and synovial fluid. J Rheumatol 1997;24:1510–6. - PubMed
-
- Usón J, Balsa A, Pascual-Salcedo D, et al. . Soluble interleukin 6 (IL-6) receptor and IL-6 levels in serum and synovial fluid of patients with different arthropathies. J Rheumatol 1997;24:2069–75. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous