

Biomarkers predict enhanced clinical outcomes with afatinib versus methotrexate in patients with second-line recurrent and/or metastatic head and neck cancer
- PMID: 28961833
- PMCID: PMC5834024
- DOI: 10.1093/annonc/mdx344
Biomarkers predict enhanced clinical outcomes with afatinib versus methotrexate in patients with second-line recurrent and/or metastatic head and neck cancer
Abstract
Background: In the phase III LUX-Head & Neck 1 (LUX-H&N1) trial, second-line afatinib significantly improved progression-free survival (PFS) versus methotrexate in patients with recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC). Here, we evaluated association of prespecified biomarkers with efficacy outcomes in LUX-H&N1.
Patients and methods: Randomized patients with R/M HNSCC and progression following ≥2 cycles of platinum therapy received afatinib (40 mg/day) or methotrexate (40 mg/m2/week). Tumor/serum samples were collected at study entry for patients who volunteered for inclusion in biomarker analyses. Tumor biomarkers, including p16 (prespecified subgroup; all tumor subsites), EGFR, HER2, HER3, c-MET and PTEN, were assessed using tissue microarray cores and slides; serum protein was evaluated using the VeriStrat® test. Biomarkers were correlated with efficacy outcomes.
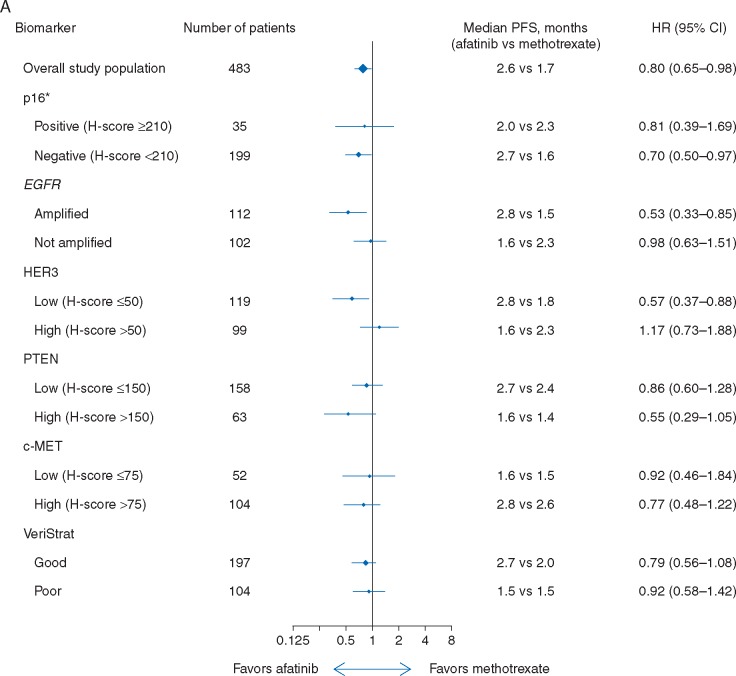
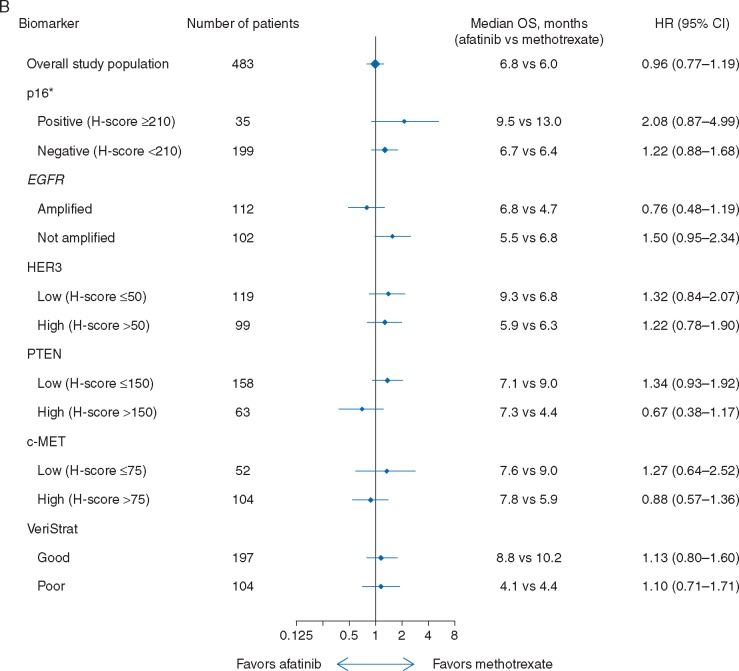
Results: Of 483 randomized patients, 326 (67%) were included in the biomarker analyses; baseline characteristics were consistent with the overall study population. Median PFS favored afatinib over methotrexate in patients with p16-negative [2.7 versus 1.6 months; HR 0.70 (95% CI 0.50-0.97)], EGFR-amplified [2.8 versus 1.5 months; HR 0.53 (0.33-0.85)], HER3-low [2.8 versus 1.8 months; HR 0.57 (0.37-0.88)], and PTEN-high [1.6 versus 1.4 months; HR 0.55 (0.29-1.05)] tumors. Afatinib also improved PFS in combined subsets of patients with p16-negative and EGFR-amplified tumors [2.7 versus 1.5 months; HR 0.47 (0.28-0.80)], and patients with p16-negative tumors who were EGFR therapy-naïve [4.0 versus 2.4 months; HR 0.55 (0.31-0.98)]. PFS was improved in afatinib-treated patients who were VeriStrat 'Good' versus 'Poor' [2.7 versus 1.5 months; HR 0.71 (0.49-0.94)], but no treatment interaction was observed. Afatinib improved tumor response versus methotrexate in all subsets analyzed except for those with p16-positive disease (n = 35).
Conclusions: Subgroups of HNSCC patients who may achieve increased benefit from afatinib were identified based on prespecified tumor biomarkers (p16-negative, EGFR-amplified, HER3-low, PTEN-high). Future studies are warranted to validate these findings.
Clinical trial registration: NCT01345682.
Keywords: EGFR; HNSCC; afatinib; biomarker; methotrexate; phase III.
© The Author 2017. Published by Oxford University Press on behalf of the European Society for Medical Oncology.
Figures
Similar articles
-
Afatinib versus methotrexate in older patients with second-line recurrent and/or metastatic head and neck squamous cell carcinoma: subgroup analysis of the LUX-Head & Neck 1 trial.Ann Oncol. 2016 Aug;27(8):1585-93. doi: 10.1093/annonc/mdw151. Epub 2016 Apr 15. Ann Oncol. 2016. PMID: 27084954 Free PMC article. Clinical Trial.
-
Afatinib versus methotrexate as second-line treatment in patients with recurrent or metastatic squamous-cell carcinoma of the head and neck progressing on or after platinum-based therapy (LUX-Head & Neck 1): an open-label, randomised phase 3 trial.Lancet Oncol. 2015 May;16(5):583-94. doi: 10.1016/S1470-2045(15)70124-5. Epub 2015 Apr 16. Lancet Oncol. 2015. PMID: 25892145 Clinical Trial.
-
Rationale and design of LUX-Head & Neck 1: a randomised, Phase III trial of afatinib versus methotrexate in patients with recurrent and/or metastatic head and neck squamous cell carcinoma who progressed after platinum-based therapy.BMC Cancer. 2014 Jun 28;14:473. doi: 10.1186/1471-2407-14-473. BMC Cancer. 2014. PMID: 24973959 Free PMC article. Clinical Trial.
-
Afatinib in squamous cell carcinoma of the head and neck.Expert Opin Pharmacother. 2016 Jun;17(9):1295-301. doi: 10.1080/14656566.2016.1183647. Epub 2016 May 19. Expert Opin Pharmacother. 2016. PMID: 27160335 Review.
-
p16(INK4a) status and survival benefit of EGFR inhibitors in head and neck squamous cell cancer: A systematic review and meta-analysis.Crit Rev Oncol Hematol. 2018 Apr;124:11-20. doi: 10.1016/j.critrevonc.2018.02.006. Epub 2018 Feb 7. Crit Rev Oncol Hematol. 2018. PMID: 29548481 Review.
Cited by
-
Identification of key genes for HNSCC from public databases using bioinformatics analysis.Cancer Cell Int. 2021 Oct 18;21(1):549. doi: 10.1186/s12935-021-02254-7. Cancer Cell Int. 2021. PMID: 34663338 Free PMC article.
-
Beyond EGFR Targeting in SCCHN: Angiogenesis, PI3K, and Other Molecular Targets.Front Oncol. 2019 Feb 13;9:74. doi: 10.3389/fonc.2019.00074. eCollection 2019. Front Oncol. 2019. PMID: 30815390 Free PMC article. Review.
-
Clinical update on head and neck cancer: molecular biology and ongoing challenges.Cell Death Dis. 2019 Jul 15;10(8):540. doi: 10.1038/s41419-019-1769-9. Cell Death Dis. 2019. PMID: 31308358 Free PMC article. Review.
-
3D cell culture alters signal transduction and drug response in head and neck squamous cell carcinoma.Oncol Lett. 2022 Jun;23(6):177. doi: 10.3892/ol.2022.13297. Epub 2022 Apr 14. Oncol Lett. 2022. PMID: 35464304 Free PMC article.
-
Investigational multitargeted kinase inhibitors in development for head and neck neoplasms.Expert Opin Investig Drugs. 2019 Apr;28(4):351-363. doi: 10.1080/13543784.2019.1581172. Epub 2019 Feb 26. Expert Opin Investig Drugs. 2019. PMID: 30753792 Free PMC article. Review.
References
-
- Machiels JP, Haddad RI, Fayette J. et al. Afatinib versus methotrexate as second-line treatment in patients with recurrent or metastatic squamous-cell carcinoma of the head and neck progressing on or after platinum-based therapy (LUX-Head & Neck 1): an open-label, randomised phase 3 trial. Lancet Oncol 2015; 16: 583–594. - PubMed
-
- Price KA, Cohen EE.. Mechanisms of and therapeutic approaches for overcoming resistance to epidermal growth factor receptor (EGFR)-targeted therapy in squamous cell carcinoma of the head and neck (SCCHN). Oral Oncol 2015; 51: 399–408. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
