

A study of the probable transmission routes of MERS-CoV during the first hospital outbreak in the Republic of Korea
- PMID: 28960494
- PMCID: PMC7165997
- DOI: 10.1111/ina.12430
A study of the probable transmission routes of MERS-CoV during the first hospital outbreak in the Republic of Korea
Abstract
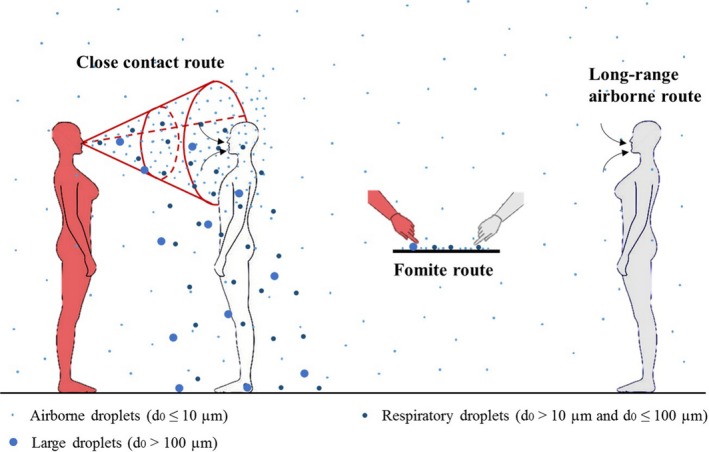
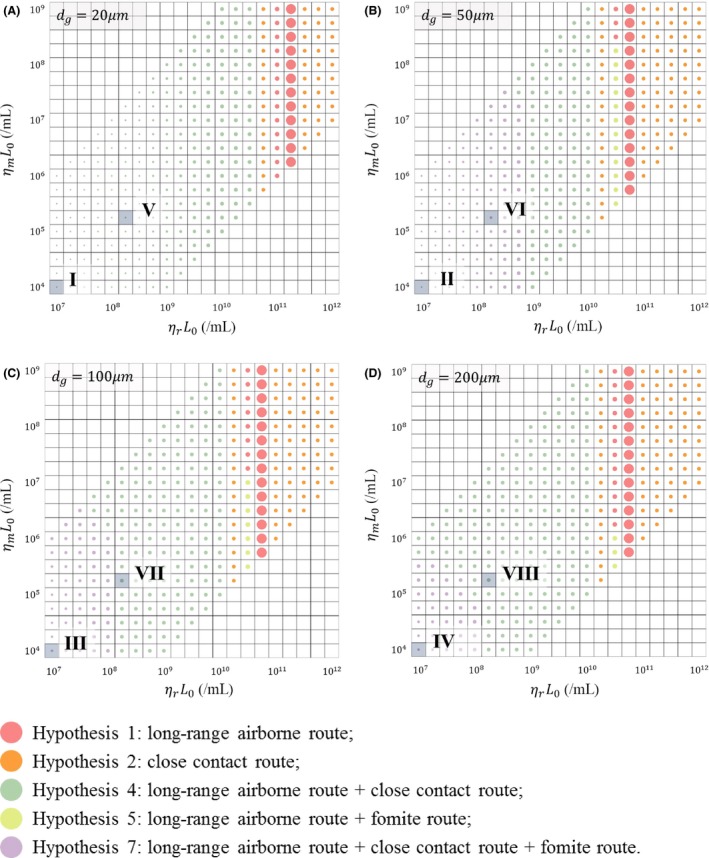
Infections caused by the Middle East respiratory syndrome coronavirus (MERS-CoV) are a serious health issue due to their prevalence and associated mortality. However, the transmission routes of the virus remain unclear, and thus, the current recommended control strategies are not evidence based. In this study, we investigated the transmission routes of MERS-CoV during the first nosocomial outbreak in the Republic of Korea in May 2015 using a multi-agent modeling framework. We identified seven hypothesized transmission modes based on the three main transmission routes (long-range airborne, close contact, and fomite). The infection risks for each hypothesis were estimated using the multi-agent modeling framework. Least-squares fitting was conducted to compare the distribution of the predicted infection risk in the various scenarios with that of the reported attack rates and to identify the hypotheses with the best fit. In the scenarios in which the index patient was a super-spreader, our model simulations suggested that MERS-CoV probably spread via the long-range airborne route. However, it is possible that the index patient shed an average viral load comparable to the loads reported in the literature, and that transmission occurred via a combined long-range airborne and close contact route.
Keywords: Fomite; Middle East respiratory syndrome coronavirus; close contact; long-range airborne; multi-agent modeling; multi-route transmission.
© 2017 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Figures

Similar articles
-
Extensive Viable Middle East Respiratory Syndrome (MERS) Coronavirus Contamination in Air and Surrounding Environment in MERS Isolation Wards.Clin Infect Dis. 2016 Aug 1;63(3):363-9. doi: 10.1093/cid/ciw239. Epub 2016 Apr 18. Clin Infect Dis. 2016. PMID: 27090992 Free PMC article.
-
Risk of transmission via medical employees and importance of routine infection-prevention policy in a nosocomial outbreak of Middle East respiratory syndrome (MERS): a descriptive analysis from a tertiary care hospital in South Korea.BMC Pulm Med. 2019 Oct 30;19(1):190. doi: 10.1186/s12890-019-0940-5. BMC Pulm Med. 2019. PMID: 31666061 Free PMC article.
-
Middle East respiratory syndrome coronavirus (MERS-CoV) outbreak in South Korea, 2015: epidemiology, characteristics and public health implications.J Hosp Infect. 2017 Feb;95(2):207-213. doi: 10.1016/j.jhin.2016.10.008. Epub 2016 Oct 14. J Hosp Infect. 2017. PMID: 28153558 Free PMC article.
-
Middle East respiratory syndrome coronavirus: current situation and travel-associated concerns.Front Med. 2016 Jun;10(2):111-9. doi: 10.1007/s11684-016-0446-y. Epub 2016 May 4. Front Med. 2016. PMID: 27146399 Free PMC article. Review.
-
Korean Society for Laboratory Medicine Practice Guidelines for the Molecular Diagnosis of Middle East Respiratory Syndrome During an Outbreak in Korea in 2015.Ann Lab Med. 2016 May;36(3):203-8. doi: 10.3343/alm.2016.36.3.203. Ann Lab Med. 2016. PMID: 26915607 Free PMC article. Review.
Cited by
-
Exploration of Superspreading Events in 2015 MERS-CoV Outbreak in Korea by Branching Process Models.Int J Environ Res Public Health. 2020 Aug 24;17(17):6137. doi: 10.3390/ijerph17176137. Int J Environ Res Public Health. 2020. PMID: 32846960 Free PMC article.
-
A Comparison of Infection Venues of COVID-19 Case Clusters in Northeast China.Int J Environ Res Public Health. 2020 Jun 3;17(11):3955. doi: 10.3390/ijerph17113955. Int J Environ Res Public Health. 2020. PMID: 32503192 Free PMC article.
-
A tracing method of airborne bacteria transmission across built environments.Build Environ. 2019 Oct 15;164:106335. doi: 10.1016/j.buildenv.2019.106335. Epub 2019 Aug 9. Build Environ. 2019. PMID: 32287991 Free PMC article.
-
Transmissibility and transmission of respiratory viruses.Nat Rev Microbiol. 2021 Aug;19(8):528-545. doi: 10.1038/s41579-021-00535-6. Epub 2021 Mar 22. Nat Rev Microbiol. 2021. PMID: 33753932 Free PMC article. Review.
-
Modeling the factors that influence exposure to SARS-CoV-2 on a subway train carriage.Indoor Air. 2022 Feb;32(2):e12976. doi: 10.1111/ina.12976. Epub 2022 Feb 8. Indoor Air. 2022. PMID: 35133673 Free PMC article. Review.
References
-
- World Health Organization . Middle East respiratory syndrome coronavirus (MERS‐CoV). [WHO website]. September 18, 2017. http://www.who.int/emergencies/mers-cov/en/. Accessed September 18, 2017.
-
- World Health Organization . WHO statement on the tenth meeting of the IHR Emergency Committee regarding MERS. [WHO website]. September 3, 2015. http://www.who.int/mediacentre/news/statements/2015/ihr-emergency-commit.... Accessed June 3, 2016.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
