

Percutaneous Image-Guided Cryoablation of Hepatic Tumors: Single-Center Experience With Intermediate to Long-Term Outcomes
- PMID: 28952807
- PMCID: PMC5698169
- DOI: 10.2214/AJR.16.17582
Percutaneous Image-Guided Cryoablation of Hepatic Tumors: Single-Center Experience With Intermediate to Long-Term Outcomes
Abstract
Objective: The purpose of this article is to report our intermediate to long-term outcomes with image-guided percutaneous hepatic tumor cryoablation and to evaluate its technical success, technique efficacy, local tumor progression, and adverse event rate.
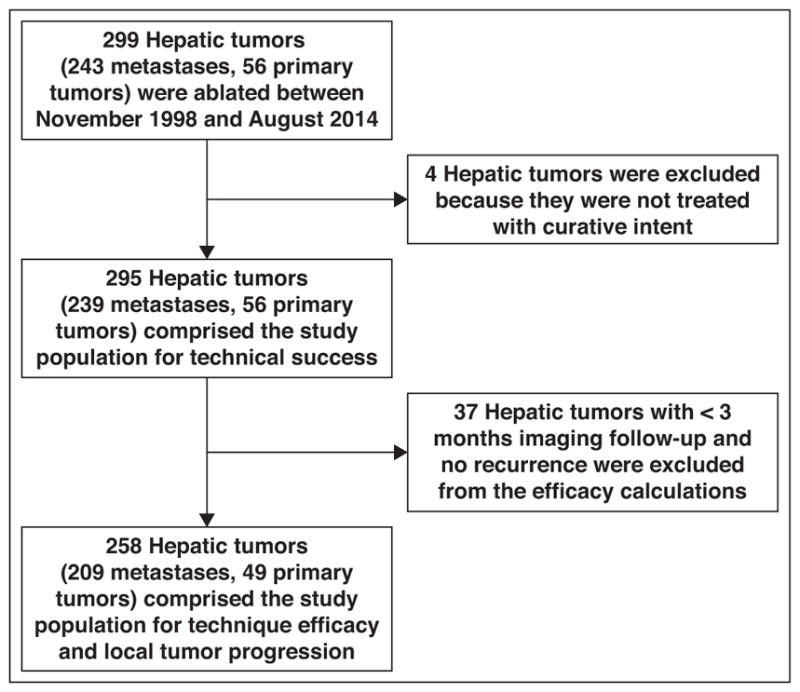
Materials and methods: Between 1998 and 2014, 299 hepatic tumors (243 metastases and 56 primary tumors; mean diameter, 2.5 cm; median diameter, 2.2 cm; range, 0.3-7.8 cm) in 186 patients (95 women; mean age, 60.9 years; range, 29-88 years) underwent cryoablation during 236 procedures using CT (n = 126), MRI (n = 100), or PET/CT (n = 10) guidance. Technical success, technique efficacy at 3 months, local tumor progression (mean follow-up, 2.5 years; range, 2 months to 14.6 years), and adverse event rates were calculated.
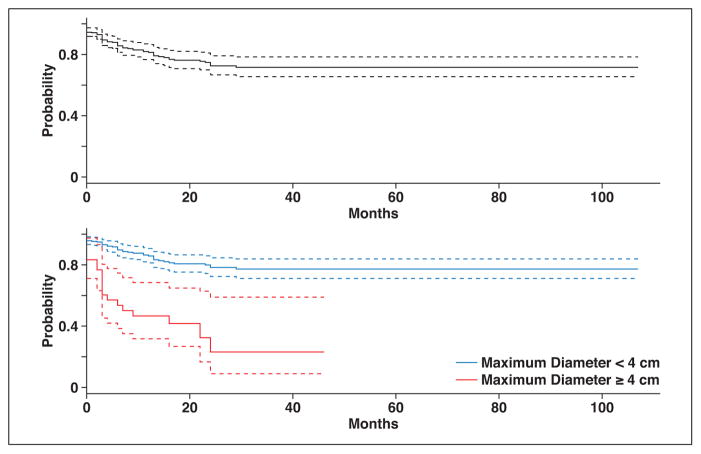
Results: The technical success rate was 94.6% (279/295). The technique efficacy rate was 89.5% (231/258) and was greater for tumors smaller than 4 cm (93.4%; 213/228) than for larger tumors (60.0%; 18/30) (p < 0.0001). Local tumor progression occurred in 23.3% (60/258) of tumors and was significantly more common after the treatment of tumors 4 cm or larger (63.3%; 19/30) compared with smaller tumors (18.0%; 41/228) (p < 0.0001). Adverse events followed 33.8% (80/236) of procedures and were grade 3-5 in 10.6% (25/236) of cases. Grade 3 or greater adverse events more commonly followed the treatment of larger tumors (19.5%; 8/41) compared with smaller tumors (8.7%; 17/195) (p = 0.04).
Conclusion: Image-guided percutaneous cryoablation of hepatic tumors is efficacious; however, tumors smaller than 4 cm are more likely to be treated successfully and without an adverse event.
Keywords: cryoablation; hepatocellular carcinoma; liver; metastases.
Figures
Comment in
-
Lollipops.AJR Am J Roentgenol. 2018 Apr;210(4):W182. doi: 10.2214/AJR.17.18959. AJR Am J Roentgenol. 2018. PMID: 29565202 No abstract available.
Similar articles
-
Percutaneous cryoablation of hepatic tumors adjacent to the gallbladder: assessment of safety and effectiveness.J Vasc Interv Radiol. 2014 Sep;25(9):1449-55. doi: 10.1016/j.jvir.2014.04.023. Epub 2014 Jun 3. J Vasc Interv Radiol. 2014. PMID: 24906627
-
Comparison of Percutaneous Image-Guided Microwave Ablation and Cryoablation for Sarcoma Lung Metastases: A 10-Year Experience.AJR Am J Roentgenol. 2022 Mar;218(3):494-504. doi: 10.2214/AJR.21.26551. Epub 2021 Oct 6. AJR Am J Roentgenol. 2022. PMID: 34612679
-
Percutaneous cryoablation of hepatic tumors: long-term experience of a large U.S. series.Abdom Radiol (NY). 2016 Apr;41(4):767-80. doi: 10.1007/s00261-016-0687-x. Abdom Radiol (NY). 2016. PMID: 26960728 Review.
-
Percutaneous imaging-guided cryoablation of liver tumors: predicting local progression on 24-hour MRI.AJR Am J Roentgenol. 2014 Aug;203(2):W181-91. doi: 10.2214/AJR.13.10747. Epub 2014 Feb 20. AJR Am J Roentgenol. 2014. PMID: 24555531
-
Image-guided percutaneous cryoablation of renal tumors.Tech Vasc Interv Radiol. 2007 Jun;10(2):140-8. doi: 10.1053/j.tvir.2007.09.009. Tech Vasc Interv Radiol. 2007. PMID: 18070692 Review.
Cited by
-
PET/CT Fluoroscopy during PET/CT-Guided Interventions: Initial Experience.J Vasc Interv Radiol. 2023 Aug;34(8):1319-1323. doi: 10.1016/j.jvir.2023.04.020. Epub 2023 May 2. J Vasc Interv Radiol. 2023. PMID: 37142215 Free PMC article.
-
Percutaneous microwave ablation of HCC: comparison between 100 and 150 W technology systems.Radiol Med. 2024 Dec;129(12):1916-1925. doi: 10.1007/s11547-024-01927-3. Epub 2024 Nov 8. Radiol Med. 2024. PMID: 39514155
-
Percutaneous Cryoablation in the Liver: A Meta-Analysis and Review of Safety with a Focus on Incidence of Cryoshock and Major Complications.Cardiovasc Intervent Radiol. 2024 Nov;47(11):1471-1484. doi: 10.1007/s00270-024-03869-9. Epub 2024 Oct 15. Cardiovasc Intervent Radiol. 2024. PMID: 39406872 Free PMC article.
-
Percutaneous cryoablation for perivascular hepatocellular carcinoma: Therapeutic efficacy and vascular complications.Eur Radiol. 2019 Feb;29(2):654-662. doi: 10.1007/s00330-018-5617-6. Epub 2018 Jul 24. Eur Radiol. 2019. PMID: 30043160
-
Cryoablation and Immunotherapy: An Enthralling Synergy to Confront the Tumors.Front Immunol. 2019 Sep 24;10:2283. doi: 10.3389/fimmu.2019.02283. eCollection 2019. Front Immunol. 2019. PMID: 31608067 Free PMC article. Review.
References
-
- American Cancer Society. Cancer facts & figures 2015. Atlanta, GA: American Cancer Society; 2015.
-
- Danet IM, Semelka RC, Leonardou P, et al. Spectrum of MRI appearances of untreated metastases of the liver. AJR. 2003;181:809–817. - PubMed
-
- Hwang M, Jayakrishnan TT, Green DE, et al. Systematic review of outcomes of patients undergoing resection for colorectal liver metastases in the setting of extra hepatic disease. Eur J Cancer. 2014;50:1747–1757. - PubMed
-
- Bala MM, Riemsma RP, Wolff R, Kleijnen J. Cryotherapy for liver metastases. Cochrane Database Syst Rev. 2013;6:CD009058. - PubMed
-
- Shin DS, Ingraham CR, Dighe MK, et al. Surgical resection of a malignant liver lesion: what the surgeon wants the radiologist to know. AJR. 2014;203:W21–W33. [web] - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
