

The predictors of 3- and 30-day mortality in 660 MERS-CoV patients
- PMID: 28893197
- PMCID: PMC5594447
- DOI: 10.1186/s12879-017-2712-2
The predictors of 3- and 30-day mortality in 660 MERS-CoV patients
Abstract
Background: The mortality rate of Middle East Respiratory Syndrome Coronavirus (MERS-CoV) patients is a major challenge in all healthcare systems worldwide. Because the MERS-CoV risk-standardized mortality rates are currently unavailable in the literature, the author concentrated on developing a method to estimate the risk-standardized mortality rates using MERS-CoV 3- and 30-day mortality measures.
Methods: MERS-CoV data in Saudi Arabia is publicly reported and made available through the Saudi Ministry of Health (SMOH) website. The author studied 660 MERS-CoV patients who were reported by the SMOH between December 2, 2014 and November 12, 2016. The data gathered contained basic demographic information (age, gender, and nationality), healthcare worker, source of infection, pre-existing illness, symptomatic, severity of illness, and regions in Saudi Arabia. The status and date of mortality were also reported. Cox-proportional hazard (CPH) models were applied to estimate the hazard ratios for the predictors of 3- and 30-day mortality.
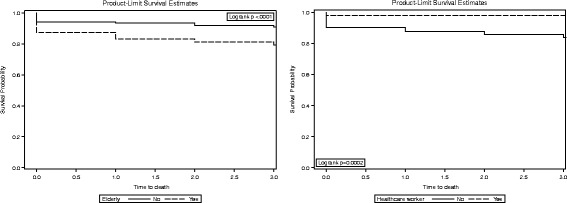
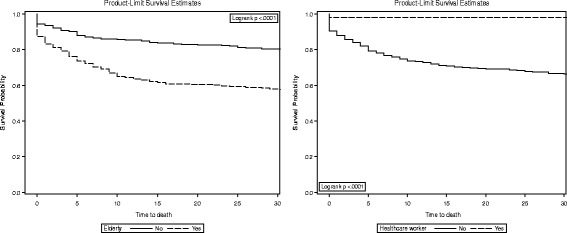
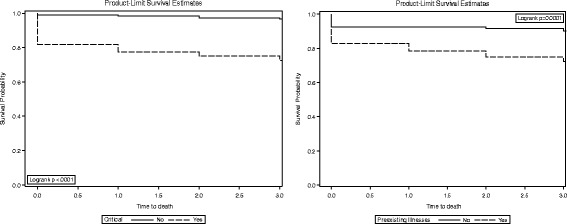
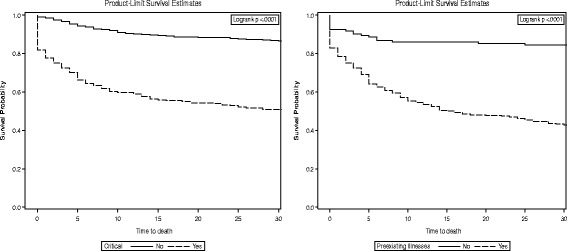
Results: 3-day, 30-day, and overall mortality were found to be 13.8%, 28.3%, and 29.8%, respectively. According to CPH, multivariate predictors of 3-day mortality were elderly, non-healthcare workers, illness severity, and hospital-acquired infections (adjusted hazard ratio (aHR) =1.7; 8.8; 6.5; and 2.8, respectively). Multivariate predictors of 30-day mortality were elderly, non-healthcare workers, pre-existing illness, severity of illness, and hospital-acquired infections (aHR =1.7; 19.2; 2.1; 3.7; and 2.9, respectively).
Conclusions: Several factors were identified that could influence mortality outcomes at 3 days and 30 days, including age (elderly), non-healthcare workers, severity of illness, and hospital-acquired infections. The findings can serve as a guide for healthcare practitioners by appropriately identifying and managing potential patients at high risk of death.
Keywords: Camels; Elderly; MERS-CoV; Mortality; Saudi Arabia.
Conflict of interest statement
Authors’ information
College of Public Health and Health Informatics, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia.
Ethics approval and consent to participate
Not applicable.
Consent for publication
The author read and approved the final manuscript.
Competing interests
The author has no competing interests to declare.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Treatment outcomes for patients with Middle Eastern Respiratory Syndrome Coronavirus (MERS CoV) infection at a coronavirus referral center in the Kingdom of Saudi Arabia.BMC Infect Dis. 2016 Apr 21;16:174. doi: 10.1186/s12879-016-1492-4. BMC Infect Dis. 2016. PMID: 27097824 Free PMC article.
-
Estimating survival rates in MERS-CoV patients 14 and 45 days after experiencing symptoms and determining the differences in survival rates by demographic data, disease characteristics and regions: a worldwide study.Epidemiol Infect. 2018 Mar;146(4):489-495. doi: 10.1017/S095026881700293X. Epub 2017 Dec 22. Epidemiol Infect. 2018. PMID: 29271336 Free PMC article.
-
An assessment of the level of concern among hospital-based health-care workers regarding MERS outbreaks in Saudi Arabia.BMC Infect Dis. 2017 Jan 3;17(1):4. doi: 10.1186/s12879-016-2096-8. BMC Infect Dis. 2017. PMID: 28049440 Free PMC article.
-
[Etiological, epidemiological and clinical aspects of coronavirus infection MERS-CoV].Pol Merkur Lekarski. 2015 Jan;38(223):46-50. Pol Merkur Lekarski. 2015. PMID: 25763589 Review. Polish.
-
Managing MERS-CoV in the healthcare setting.Hosp Pract (1995). 2015;43(3):158-63. doi: 10.1080/21548331.2015.1074029. Hosp Pract (1995). 2015. PMID: 26224424 Review.
Cited by
-
A Predictive Nomogram for Predicting Improved Clinical Outcome Probability in Patients with COVID-19 in Zhejiang Province, China.Engineering (Beijing). 2022 Jan;8:122-129. doi: 10.1016/j.eng.2020.05.014. Epub 2020 Jun 6. Engineering (Beijing). 2022. PMID: 32837744 Free PMC article.
-
Climate factors and incidence of Middle East respiratory syndrome coronavirus.J Infect Public Health. 2020 May;13(5):704-708. doi: 10.1016/j.jiph.2019.11.011. Epub 2019 Dec 6. J Infect Public Health. 2020. PMID: 31813836 Free PMC article.
-
Predictors of mortality in patients with coronavirus disease 2019: a systematic review and meta-analysis.BMC Infect Dis. 2021 Jul 8;21(1):663. doi: 10.1186/s12879-021-06369-0. BMC Infect Dis. 2021. PMID: 34238232 Free PMC article.
-
The effects of aging on host resistance and disease tolerance to SARS-CoV-2 infection.FEBS J. 2021 Sep;288(17):5055-5070. doi: 10.1111/febs.15613. Epub 2020 Nov 17. FEBS J. 2021. PMID: 33124149 Free PMC article. Review.
-
Comorbid diabetes results in immune dysregulation and enhanced disease severity following MERS-CoV infection.JCI Insight. 2019 Oct 17;4(20):e131774. doi: 10.1172/jci.insight.131774. JCI Insight. 2019. PMID: 31550243 Free PMC article.
References
-
- World Health Organization. Middle East respiratory syndrome coronavirus (MERS-CoV): summary of current situation, literature update and risk assessment. (Accessed 22 Nov 2016 at http://www.who.int/emergencies/mers-cov/en/.)
-
- Khan K, Sears J, Hu VW, Brownstein JS, Hay S, Kossowsky D, Eckhardt R, Chim T, Berry I, Bogoch I, Cetron M. Potential for the International Spread of Middle East Respiratory Syndrome in Association with Mass Gatherings in Saudi Arabia. PLOS Currents Outbreaks. 2013 Jul 17 . Edition 1. doi:10.1371/currents.outbreaks.a7b70897ac2fa4f79b59f90d24c860b8. - PMC - PubMed
-
- Assiri A, Al-Tawfiq JA, Al-Rabeeah AA, et al. Epidemiological, demographic, and clinical characteristics of 47 cases of Middle East respiratory syndrome coronavirus disease from Saudi Arabia: a descriptive study. Lancet Infect Dis. 2013;13(9):752–761. doi: 10.1016/S1473-3099(13)70204-4. - DOI - PMC - PubMed
-
- Noorwali AA, Turkistani AM, Asiri SI, et al. Descriptive epidemiology and characteristics of confirmed cases of Middle East respiratory syndrome coronavirus infection in the Makkah Region of Saudi Arabia, March to June 2014. Annals of Saudi medicine. 2015;35(3):203. doi: 10.5144/0256-4947.2015.203. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
