

Human Immunodeficiency Virus Type 1 Persistence Following Systemic Chemotherapy for Malignancy
- PMID: 28838149
- PMCID: PMC5853412
- DOI: 10.1093/infdis/jix265
Human Immunodeficiency Virus Type 1 Persistence Following Systemic Chemotherapy for Malignancy
Abstract
Background: Systemic chemotherapies for various malignancies have been shown to significantly, yet transiently, decrease numbers of CD4+ T lymphocytes, a major reservoir for human immunodeficiency virus type 1 (HIV-1) infection. However, little is known about the impact of cytoreductive chemotherapy on HIV-1 reservoir dynamics, persistence, and immune responses.
Methods: We investigated the changes in peripheral CD4+ T-cell-associated HIV-1 DNA and RNA levels, lymphocyte activation, viral population structure, and virus-specific immune responses in a longitudinal cohort of 15 HIV-1-infected individuals receiving systemic chemotherapy or subsequent autologous stem cell transplantation for treatment of hematological malignancies and solid tumors.
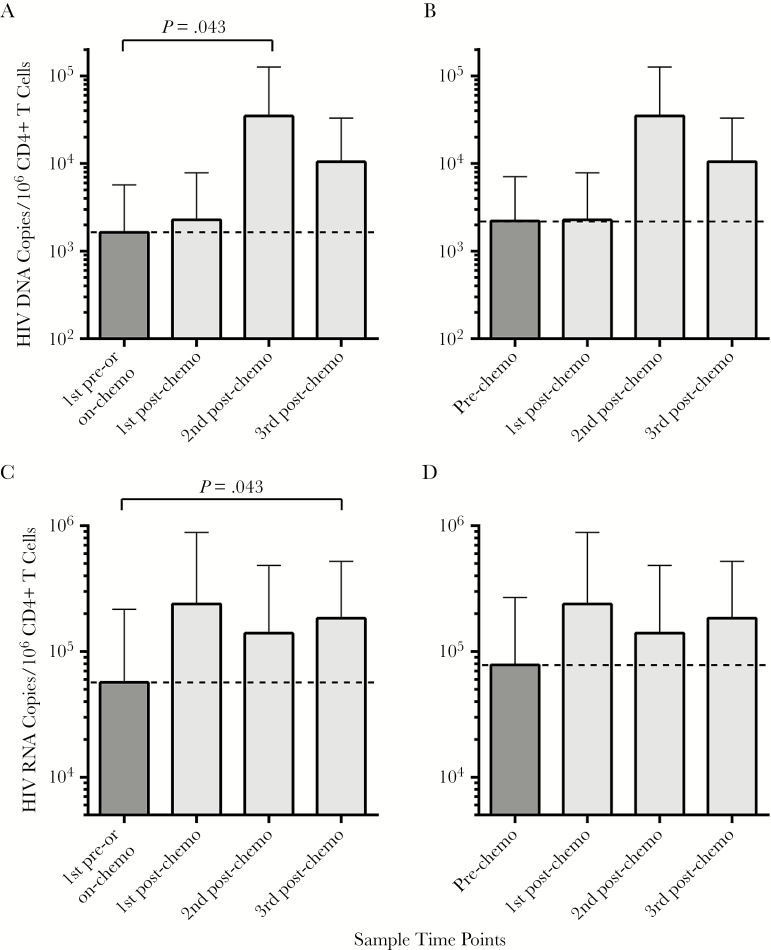
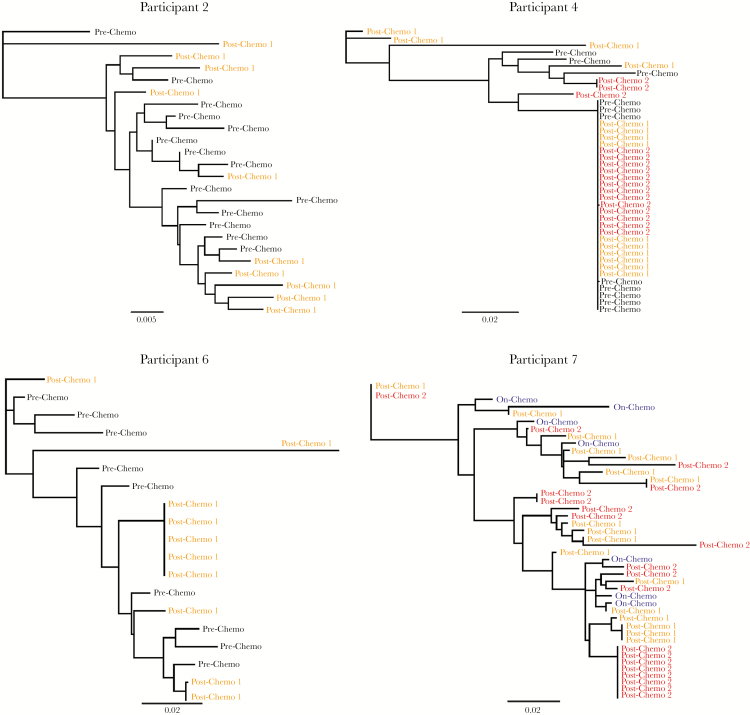
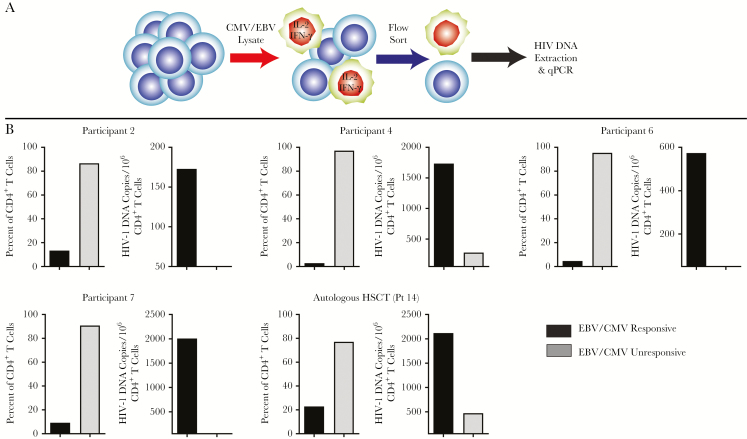
Results: Despite a transient reduction in CD4+ T cells capable of harboring HIV-1, a 1.7- and 3.3-fold increase in mean CD4+ T-cell-associated HIV-1 RNA and DNA, respectively, were observed months following completion of chemotherapy in individuals on antiretroviral therapy. We also observed changes in CD4+ T-cell population diversity and clonal viral sequence expansion during CD4+ T-cell reconstitution following chemotherapy cessation. Finally, HIV-1 DNA was preferentially, and in some cases exclusively, detected in cytomegalovirus (CMV)- and Epstein-Barr virus (EBV)-responsive CD4+ T cells following chemotherapy.
Conclusions: Expansion of HIV-infected CMV/EBV-specific CD4 + T cells may contribute to maintenance of the HIV DNA reservoir following chemotherapy.
Keywords: HIV-1; chemotherapy; cytomegalovirus infection; lymphoma; stem cell transplantation.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Asymptomatic CMV Replication During Early Human Immunodeficiency Virus (HIV) Infection Is Associated With Lower CD4/CD8 Ratio During HIV Treatment.Clin Infect Dis. 2016 Dec 1;63(11):1517-1524. doi: 10.1093/cid/ciw612. Epub 2016 Sep 6. Clin Infect Dis. 2016. PMID: 27601222 Free PMC article.
-
Subclinical Cytomegalovirus DNA Is Associated with CD4 T Cell Activation and Impaired CD8 T Cell CD107a Expression in People Living with HIV despite Early Antiretroviral Therapy.J Virol. 2019 Jun 14;93(13):e00179-19. doi: 10.1128/JVI.00179-19. Print 2019 Jul 1. J Virol. 2019. PMID: 31019052 Free PMC article.
-
Subclinical Cytomegalovirus and Epstein-Barr Virus Shedding Is Associated with Increasing HIV DNA Molecular Diversity in Peripheral Blood during Suppressive Antiretroviral Therapy.J Virol. 2020 Sep 15;94(19):e00927-20. doi: 10.1128/JVI.00927-20. Print 2020 Sep 15. J Virol. 2020. PMID: 32641485 Free PMC article.
-
Reservoirs for HIV-1: mechanisms for viral persistence in the presence of antiviral immune responses and antiretroviral therapy.Annu Rev Immunol. 2000;18:665-708. doi: 10.1146/annurev.immunol.18.1.665. Annu Rev Immunol. 2000. PMID: 10837072 Review.
-
Cytomegalovirus and HIV Persistence: Pouring Gas on the Fire.AIDS Res Hum Retroviruses. 2017 Nov;33(S1):S23-S30. doi: 10.1089/aid.2017.0145. AIDS Res Hum Retroviruses. 2017. PMID: 29140108 Free PMC article. Review.
Cited by
-
Atherosclerosis and Cardiovascular Complications in People Living with HIV: A Focused Review.Infect Dis Rep. 2024 Sep 1;16(5):846-863. doi: 10.3390/idr16050066. Infect Dis Rep. 2024. PMID: 39311207 Free PMC article. Review.
-
Spatial technologies to evaluate the HIV-1 reservoir and its microenvironment in the lymph node.mBio. 2024 Aug 14;15(8):e0190924. doi: 10.1128/mbio.01909-24. Epub 2024 Jul 26. mBio. 2024. PMID: 39058091 Free PMC article. Review.
-
Gaining momentum: stem cell therapies for HIV cure.Curr Opin HIV AIDS. 2024 Jul 1;19(4):194-200. doi: 10.1097/COH.0000000000000859. Epub 2024 Apr 26. Curr Opin HIV AIDS. 2024. PMID: 38686850 Free PMC article. Review.
-
The latent reservoir of inducible, infectious HIV-1 does not decrease despite decades of antiretroviral therapy.J Clin Invest. 2023 Sep 1;133(17):e171554. doi: 10.1172/JCI171554. J Clin Invest. 2023. PMID: 37463049 Free PMC article.
-
Antigen specificities of HIV-infected cells: A role in infection and persistence?J Virus Erad. 2023 Jun 1;9(2):100329. doi: 10.1016/j.jve.2023.100329. eCollection 2023 Jun. J Virus Erad. 2023. PMID: 37440870 Free PMC article. Review.
References
-
- Siliciano JD, Kajdas J, Finzi D et al. . Long-term follow-up studies confirm the stability of the latent reservoir for HIV-1 in resting CD4+ T cells. Nat Med 2003; 9:727–8. - PubMed
-
- Chun TW, Justement JS, Moir S et al. . Decay of the HIV reservoir in patients receiving antiretroviral therapy for extended periods: implications for eradication of virus. J Infect Dis 2007; 195:1762–4. - PubMed
-
- Mackall CL, Fleisher TA, Brown MR et al. . Lymphocyte depletion during treatment with intensive chemotherapy for cancer. Blood 1994; 84:2221–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
