

Regulation of human airway smooth muscle cell migration and relevance to asthma
- PMID: 28814293
- PMCID: PMC5559796
- DOI: 10.1186/s12931-017-0640-8
Regulation of human airway smooth muscle cell migration and relevance to asthma
Abstract
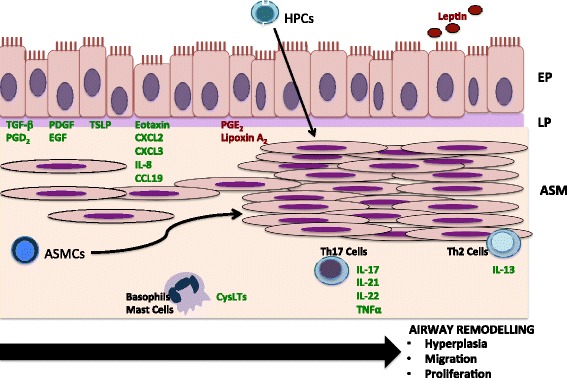
Airway remodelling is an important feature of asthma pathogenesis. A key structural change inherent in airway remodelling is increased airway smooth muscle mass. There is emerging evidence to suggest that the migration of airway smooth muscle cells may contribute to cellular hyperplasia, and thus increased airway smooth muscle mass. The precise source of these cells remains unknown. Increased airway smooth muscle mass may be collectively due to airway infiltration of myofibroblasts, neighbouring airway smooth muscle cells in the bundle, or circulating hemopoietic progenitor cells. However, the relative contribution of each cell type is not well understood. In addition, although many studies have identified pro and anti-migratory agents of airway smooth muscle cells, whether these agents can impact airway remodelling in the context of human asthma, remains to be elucidated. As such, further research is required to determine the exact mechanism behind airway smooth muscle cell migration within the airways, how much this contributes to airway smooth muscle mass in asthma, and whether attenuating this migration may provide a therapeutic avenue for asthma. In this review article, we will discuss the current evidence with respect to the regulation of airway smooth muscle cell migration in asthma.
Keywords: Airway smooth muscle; Asthma; Cytokines; Migration; Remodelling.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Origins of increased airway smooth muscle mass in asthma.BMC Med. 2013 Jun 6;11:145. doi: 10.1186/1741-7015-11-145. BMC Med. 2013. PMID: 23742314 Free PMC article. Review.
-
TH17 cytokines induce human airway smooth muscle cell migration.J Allergy Clin Immunol. 2011 Apr;127(4):1046-53.e1-2. doi: 10.1016/j.jaci.2010.12.1117. Epub 2011 Feb 22. J Allergy Clin Immunol. 2011. PMID: 21345484
-
STAT3 potentiates the ability of airway smooth muscle cells to promote angiogenesis by regulating VEGF signalling.Exp Physiol. 2017 May 1;102(5):598-606. doi: 10.1113/EP086136. Epub 2017 Apr 7. Exp Physiol. 2017. PMID: 28295786
-
Neuronal chemorepellent Semaphorin 3E inhibits human airway smooth muscle cell proliferation and migration.J Allergy Clin Immunol. 2014 Feb;133(2):560-7. doi: 10.1016/j.jaci.2013.06.011. Epub 2013 Aug 6. J Allergy Clin Immunol. 2014. PMID: 23932461
-
Airway smooth muscle growth in asthma: proliferation, hypertrophy, and migration.Proc Am Thorac Soc. 2008 Jan 1;5(1):89-96. doi: 10.1513/pats.200705-063VS. Proc Am Thorac Soc. 2008. PMID: 18094090 Free PMC article. Review.
Cited by
-
Research advances in airway remodeling in asthma: a narrative review.Ann Transl Med. 2022 Sep;10(18):1023. doi: 10.21037/atm-22-2835. Ann Transl Med. 2022. PMID: 36267708 Free PMC article. Review.
-
Biological Therapies of Severe Asthma and Their Possible Effects on Airway Remodeling.Front Immunol. 2020 Jun 18;11:1134. doi: 10.3389/fimmu.2020.01134. eCollection 2020. Front Immunol. 2020. PMID: 32625205 Free PMC article. Review.
-
β-Tocotrienol Decreases PDGF-BB-Induced Proliferation and Migration of Human Airway Smooth Muscle Cells by Inhibiting RhoA and Reducing ROS Production.Pharmaceuticals (Basel). 2024 May 30;17(6):712. doi: 10.3390/ph17060712. Pharmaceuticals (Basel). 2024. PMID: 38931379 Free PMC article.
-
Cell-Specific DNA Methylation Signatures in Asthma.Genes (Basel). 2019 Nov 15;10(11):932. doi: 10.3390/genes10110932. Genes (Basel). 2019. PMID: 31731604 Free PMC article. Review.
-
Differential Expression of lncRNA CASC2 in the Serum of Childhood Asthma and Its Role in Airway Smooth Muscle Cells Proliferation and Migration.J Asthma Allergy. 2022 Feb 11;15:197-207. doi: 10.2147/JAA.S337236. eCollection 2022. J Asthma Allergy. 2022. PMID: 35185342 Free PMC article.
References
-
- Huber HL, Koessler KK. The pathology of bronchial asthma. Arch Intern Med. 1922;30:689–760. doi: 10.1001/archinte.1922.00110120002001. - DOI
-
- Heard BE, Hossain S. Hyperplasia of bronchial smooth muscle in asthma. J Pathol. 1973;110:319–312. doi: 10.1002/path.1711100406. - DOI
-
- Sobonya RE. Quantitative structural alterations in long-standing allergic asthma. Am Rev Respir Dis. 1984;130:289–292. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
