

Association of Coffee Consumption With Total and Cause-Specific Mortality Among Nonwhite Populations
- PMID: 28693036
- PMCID: PMC7494322
- DOI: 10.7326/M16-2472
Association of Coffee Consumption With Total and Cause-Specific Mortality Among Nonwhite Populations
Abstract
Background: Coffee consumption has been associated with reduced risk for death in prospective cohort studies; however, data in nonwhites are sparse.
Objective: To examine the association of coffee consumption with risk for total and cause-specific death.
Design: The MEC (Multiethnic Cohort), a prospective population-based cohort study established between 1993 and 1996.
Setting: Hawaii and Los Angeles, California.
Participants: 185 855 African Americans, Native Hawaiians, Japanese Americans, Latinos, and whites aged 45 to 75 years at recruitment.
Measurements: Outcomes were total and cause-specific mortality between 1993 and 2012. Coffee intake was assessed at baseline by means of a validated food-frequency questionnaire.
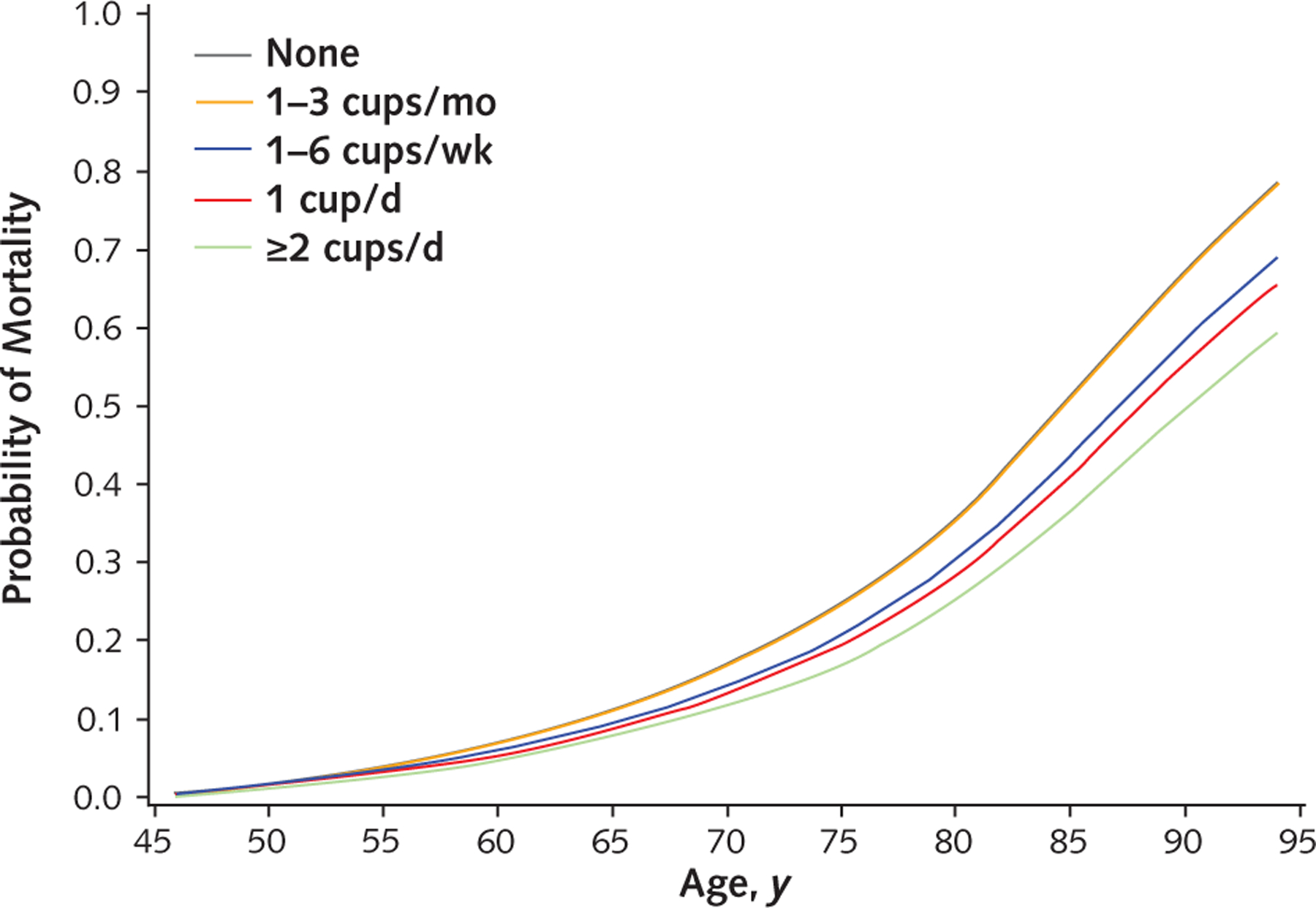
Results: 58 397 participants died during 3 195 484 person-years of follow-up (average follow-up, 16.2 years). Compared with drinking no coffee, coffee consumption was associated with lower total mortality after adjustment for smoking and other potential confounders (1 cup per day: hazard ratio [HR], 0.88 [95% CI, 0.85 to 0.91]; 2 to 3 cups per day: HR, 0.82 [CI, 0.79 to 0.86]; ≥4 cups per day: HR, 0.82 [CI, 0.78 to 0.87]; P for trend < 0.001). Trends were similar between caffeinated and decaffeinated coffee. Significant inverse associations were observed in 4 ethnic groups; the association in Native Hawaiians did not reach statistical significance. Inverse associations were also seen in never-smokers, younger participants (<55 years), and those who had not previously reported a chronic disease. Among examined end points, inverse associations were observed for deaths due to heart disease, cancer, respiratory disease, stroke, diabetes, and kidney disease.
Limitation: Unmeasured confounding and measurement error, although sensitivity analysis suggested that neither was likely to affect results.
Conclusion: Higher consumption of coffee was associated with lower risk for death in African Americans, Japanese Americans, Latinos, and whites.
Primary funding source: National Cancer Institute.
Conflict of interest statement
Figures
Comment in
-
Coffee Drinking and Mortality in 10 European Countries.Ann Intern Med. 2018 Mar 6;168(5):379-380. doi: 10.7326/L17-0687. Ann Intern Med. 2018. PMID: 29507961 No abstract available.
-
Coffee Drinking and Mortality in 10 European Countries.Ann Intern Med. 2018 Mar 6;168(5):380-381. doi: 10.7326/L17-0689. Ann Intern Med. 2018. PMID: 29507963 No abstract available.
Similar articles
-
Association of coffee intake with reduced incidence of liver cancer and death from chronic liver disease in the US multiethnic cohort.Gastroenterology. 2015 Jan;148(1):118-25; quiz e15. doi: 10.1053/j.gastro.2014.10.005. Epub 2014 Oct 8. Gastroenterology. 2015. PMID: 25305507 Free PMC article.
-
Prospective Study of Coffee Consumption and Cancer Incidence in Non-White Populations.Cancer Epidemiol Biomarkers Prev. 2018 Aug;27(8):928-935. doi: 10.1158/1055-9965.EPI-18-0093. Epub 2018 May 18. Cancer Epidemiol Biomarkers Prev. 2018. PMID: 29777049 Free PMC article.
-
Weight change in older adults and mortality: the Multiethnic Cohort Study.Int J Obes (Lond). 2018 Feb;42(2):205-212. doi: 10.1038/ijo.2017.188. Epub 2017 Aug 14. Int J Obes (Lond). 2018. PMID: 28885999 Free PMC article.
-
Association of Coffee Consumption With Total and Cause-Specific Mortality in 3 Large Prospective Cohorts.Circulation. 2015 Dec 15;132(24):2305-15. doi: 10.1161/CIRCULATIONAHA.115.017341. Epub 2015 Nov 16. Circulation. 2015. PMID: 26572796 Free PMC article.
-
Association of coffee drinking with total and cause-specific mortality.N Engl J Med. 2012 May 17;366(20):1891-904. doi: 10.1056/NEJMoa1112010. N Engl J Med. 2012. PMID: 22591295 Free PMC article.
Cited by
-
A Healthy Beverage Score and Risk of Chronic Kidney Disease Progression, Incident Cardiovascular Disease, and All-Cause Mortality in the Chronic Renal Insufficiency Cohort.Curr Dev Nutr. 2020 May 21;4(6):nzaa088. doi: 10.1093/cdn/nzaa088. eCollection 2020 Jun. Curr Dev Nutr. 2020. PMID: 32551412 Free PMC article.
-
Chronic low-grade inflammation associated with higher risk and earlier onset of cardiometabolic multimorbidity in middle-aged and older adults: a population-based cohort study.Sci Rep. 2024 Sep 30;14(1):22635. doi: 10.1038/s41598-024-72988-7. Sci Rep. 2024. PMID: 39349699 Free PMC article.
-
Appraisal of the causal effect of plasma caffeine on adiposity, type 2 diabetes, and cardiovascular disease: two sample mendelian randomisation study.BMJ Med. 2023 Jan 31;2(1):1-8. doi: 10.1136/bmjmed-2022-000335. eCollection 2023. BMJ Med. 2023. PMID: 36936261 Free PMC article.
-
Effect of Prehospital Epinephrine Use on Survival from Out-of-Hospital Cardiac Arrest and on Emergency Medical Services.J Clin Med. 2021 Dec 30;11(1):190. doi: 10.3390/jcm11010190. J Clin Med. 2021. PMID: 35011931 Free PMC article.
-
Association of serum copper (Cu) with cardiovascular mortality and all-cause mortality in a general population: a prospective cohort study.BMC Public Health. 2023 Nov 1;23(1):2138. doi: 10.1186/s12889-023-17018-3. BMC Public Health. 2023. PMID: 37915007 Free PMC article.
References
-
- Huxley R, Lee CM, Barzi F, Timmermeister L, Czernichow S, Perkovic V, et al. Coffee, decaffeinated coffee, and tea consumption in relation to incident type 2 diabetes mellitus: a systematic review with meta-analysis. Arch Intern Med. 2009;169:2053–63. doi:10.1001/archinternmed.2009.439 - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources