

Advances in keratinocyte delivery in burn wound care
- PMID: 28668483
- PMCID: PMC5764224
- DOI: 10.1016/j.addr.2017.06.012
Advances in keratinocyte delivery in burn wound care
Abstract
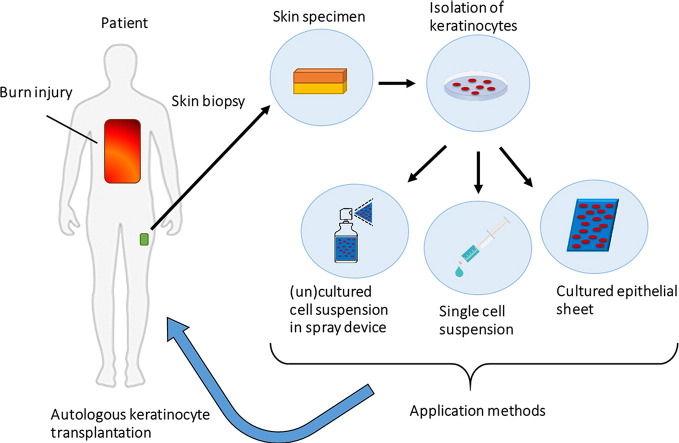
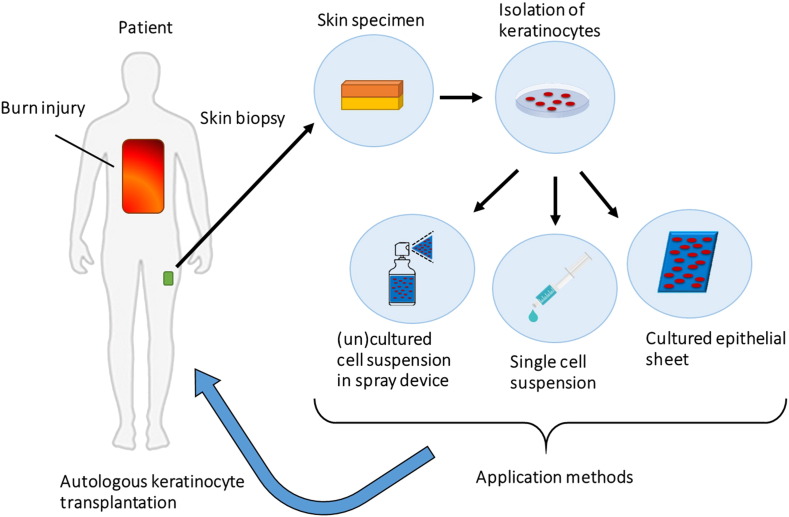
This review gives an updated overview on keratinocyte transplantation in burn wounds concentrating on application methods and future therapeutic cell delivery options with a special interest in hydrogels and spray devices for cell delivery. To achieve faster re-epithelialisation of burn wounds, the original autologous keratinocyte culture and transplantation technique was introduced over 3 decades ago. Application types of keratinocytes transplantation have improved from cell sheets to single-cell solutions delivered with a spray system. However, further enhancement of cell culture, cell viability and function in vivo, cell carrier and cell delivery systems remain themes of interest. Hydrogels such as chitosan, alginate, fibrin and collagen are frequently used in burn wound care and have advantageous characteristics as cell carriers. Future approaches of keratinocyte transplantation involve spray devices, but optimisation of application technique and carrier type is necessary.
Keywords: Burn injury; Cell transplantation; Hydrogels; Spray application; Wound healing.
Copyright © 2017 The Author(s). Published by Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Preparation and characterization of human keratinocyte-fibroblast cell sheets constructed using PNIAM-co-AM grafted surfaces for burn wound healing.J Mater Sci Mater Med. 2020 Nov 28;31(12):126. doi: 10.1007/s10856-020-06469-4. J Mater Sci Mater Med. 2020. PMID: 33247815
-
A comparison of keratinocyte cell sprays with and without fibrin glue.Burns. 2003 Nov;29(7):677-85. doi: 10.1016/s0305-4179(03)00155-4. Burns. 2003. PMID: 14556725
-
In vitro transfer of keratinocytes: comparison of transfer from fibrin membrane and delivery by aerosol spray.J Biomed Mater Res B Appl Biomater. 2005 May;73(2):221-8. doi: 10.1002/jbm.b.30198. J Biomed Mater Res B Appl Biomater. 2005. PMID: 15772966
-
A review of keratinocyte delivery to the wound bed.J Burn Care Rehabil. 2004 May-Jun;25(3):266-75. doi: 10.1097/01.bcr.0000124749.85552.cd. J Burn Care Rehabil. 2004. PMID: 15273468 Review.
-
[Application of autologous and allogenic keratynocyte cultures in burn management].Przegl Lek. 2005;62(9):934-7. Przegl Lek. 2005. PMID: 16541733 Review. Polish.
Cited by
-
Alternative therapeutic strategies in diabetes management.World J Diabetes. 2024 Jun 15;15(6):1142-1161. doi: 10.4239/wjd.v15.i6.1142. World J Diabetes. 2024. PMID: 38983831 Free PMC article. Review.
-
Drug Repurposing for Atopic Dermatitis by Integration of Gene Networking and Genomic Information.Front Immunol. 2021 Oct 13;12:724277. doi: 10.3389/fimmu.2021.724277. eCollection 2021. Front Immunol. 2021. PMID: 34721386 Free PMC article.
-
Xeno-free workflow exhibits comparable efficiency and quality of keratinocytes isolated from human skin biopsies.Regen Ther. 2021 Sep 29;18:401-407. doi: 10.1016/j.reth.2021.09.005. eCollection 2021 Dec. Regen Ther. 2021. PMID: 34722836 Free PMC article.
-
Effect of Crosslinking Type on the Physical-Chemical Properties and Biocompatibility of Chitosan-Based Electrospun Membranes.Polymers (Basel). 2021 Mar 9;13(5):831. doi: 10.3390/polym13050831. Polymers (Basel). 2021. PMID: 33803084 Free PMC article.
-
Impact of human mesenchymal cells of different body site origins on the maturation of dermo-epidermal skin substitutes.Pediatr Surg Int. 2019 Jan;35(1):121-127. doi: 10.1007/s00383-018-4383-5. Epub 2018 Oct 31. Pediatr Surg Int. 2019. PMID: 30382375
References
-
- Jackson P.C., Hardwicke J., Bamford A., Nightingale P., Wilson Y., Papini R. Revised estimates of mortality from the Birmingham Burn Centre, 2001–2010: a continuing analysis over 65 years. Ann. Surg. 2014;259(5):979–984. - PubMed
-
- Web-based injury statistics query and reporting system [Internet] 2014. https://www.cdc.gov/injury/wisqars/ [cited 06/10/2016]. Available from: - PubMed
-
- Osler T., Glance L.G., Hosmer D.W. Simplified estimates of the probability of death after burn injuries: extending and updating the Baux score. J. Trauma. 2010;68(3):690–697. - PubMed
-
- Tobiasen J., Hiebert J.M., Edlich R.F. The abbreviated burn severity index. Ann. Emerg. Med. 1982;11(5):260–262. - PubMed
-
- Muller M.J., Herndon D.N. The challenge of burns. Lancet (London, England) 1994;343(8891):216–220. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
