

Contemporary Diagnostic Imaging of Oral Squamous Cell Carcinoma - A Review of Literature
- PMID: 28439324
- PMCID: PMC5391802
- DOI: 10.12659/PJR.900892
Contemporary Diagnostic Imaging of Oral Squamous Cell Carcinoma - A Review of Literature
Abstract
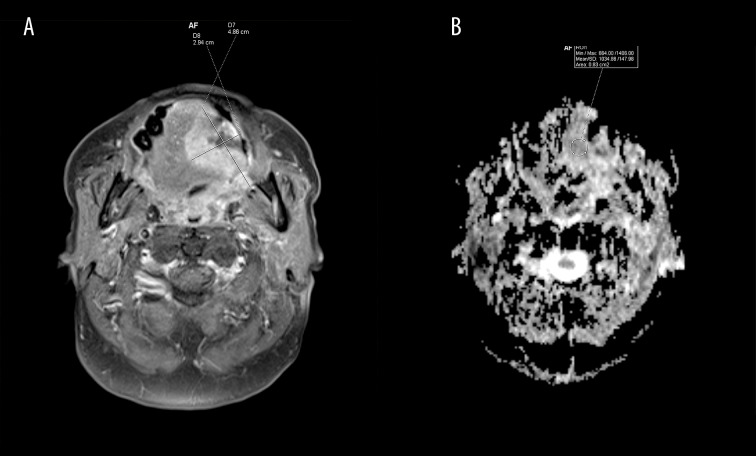
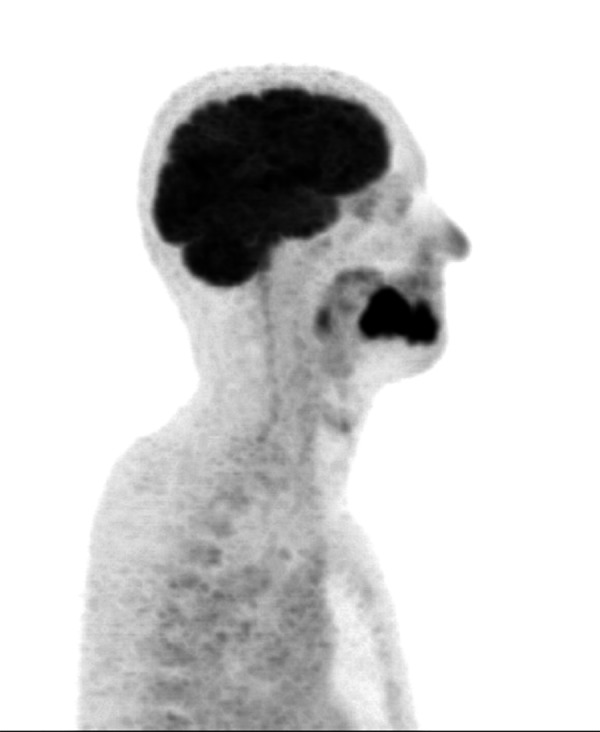
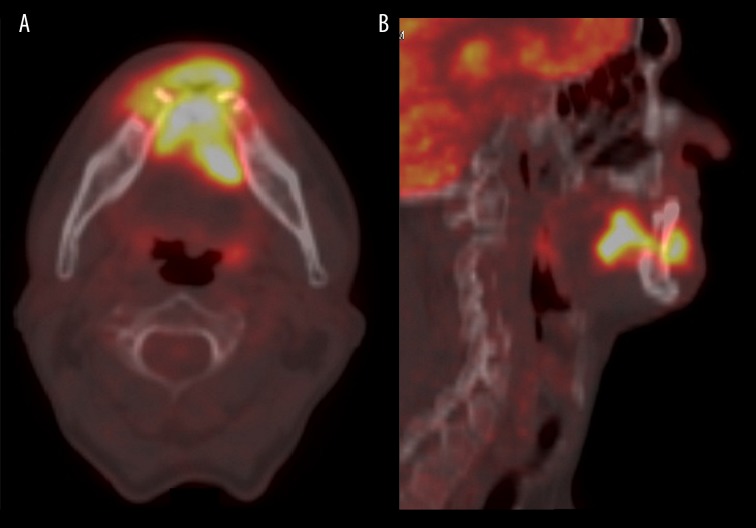
Oral squamous cell carcinoma (OSCC) is the most common cancer of the oral cavity and constitutes 95% of all cancers of this area. Men are affected twice as commonly as women, primarily if they are over 50 years of age. Forty percent of the lesions are localized in the tongue and 30% in the floor of the oral cavity. OSCC often affects upper and lower gingiva, buccal mucous membrane, the retromolar triangle and the palate. The prognosis is poor and the five-year survival rate ranges from 20% (OSCC in the floor of the mouth) to 60% (OSCC in the alveolar part of the mandible). Treatment is difficult, because of the localization and the invasiveness of the available methods. The diagnosis is made based on a histopathological examination of a biopsy sample. The low detection rate of early oral SCC is a considerable clinical issue. Although the oral cavity can be easily examined, in the majority of cases oral SCC is diagnosed in its late stages. It is difficult to diagnose metastases in local lymph nodes and distant organs, which is important for planning the scope of resection and further treatment, graft implantation, and differentiation between reactive and metastatic lymph nodes as well as between disease recurrence and scars or adverse reactions after surgery or radiation therapy. Imaging studies are performed as part of the routine work-up in oral SCC. However, it is difficult to interpret the results at the early stages of the disease. The following imaging methods are used - dental radiographs, panoramic radiographs, magnetic resonance imaging with diffusion-weighted and dynamic sequences, perfusion computed tomography, cone beam computed tomography, single-photon emission computed tomography, hybrid methods (PET/CT, PET/MRI, SPECT/CT) and ultrasound. Some important clinical problems can be resolved with the use of novel modalities such as MRI with ADC sequences and PET. The aim of this article is to describe oral squamous cell carcinoma as it appears in different imaging methods considering both their advantages and limitations.
Keywords: Carcinoma, Squamous Cell; Cone-Beam Computed Tomography; Diagnostic Imaging; Diffusion Magnetic Resonance Imaging; Perfusion Imaging.
Figures

Similar articles
-
Oral cavity squamous cell carcinoma: role of pretreatment imaging and its influence on management.Clin Radiol. 2014 Sep;69(9):916-30. doi: 10.1016/j.crad.2014.04.013. Epub 2014 Jun 5. Clin Radiol. 2014. PMID: 24908285
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Prospective evaluation of outcome after transoral CO(2) laser resection of T1/T2 oral squamous cell carcinoma.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 Aug;112(2):180-7. doi: 10.1016/j.tripleo.2010.09.078. Epub 2011 Jan 12. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011. PMID: 21232996
-
Utility of imaging techniques in the diagnosis of oral cancer.J Craniomaxillofac Surg. 2015 Nov;43(9):1880-94. doi: 10.1016/j.jcms.2015.07.037. Epub 2015 Aug 7. J Craniomaxillofac Surg. 2015. PMID: 26325616 Review.
-
The role of ultrasound in primary workup of cervical cancer staging (ESGO, ESTRO, ESP cervical cancer guidelines).Ceska Gynekol. 2019 Winter;84(1):40-48. Ceska Gynekol. 2019. PMID: 31213057 Review. English.
Cited by
-
The diagnostic yield of preoperative screening for oral cancer in dogs over 15 years, part 1: locoregional screening.J Am Vet Med Assoc. 2023 Sep 29;261(S2):S14-S23. doi: 10.2460/javma.23.05.0299. Print 2023 Dec 1. J Am Vet Med Assoc. 2023. PMID: 37863103 Free PMC article.
-
An Unusual Case of Mandibular Squamous Cell Carcinoma in Intimacy with an Impacted Wisdom Tooth.Case Rep Surg. 2019 Apr 11;2019:8360357. doi: 10.1155/2019/8360357. eCollection 2019. Case Rep Surg. 2019. PMID: 31110834 Free PMC article.
-
Clinical practice guidelines for radiographic assessment in management of oral cancer.J Adv Pharm Technol Res. 2022 Oct-Dec;13(4):248-251. doi: 10.4103/japtr.japtr_129_22. Epub 2022 Oct 10. J Adv Pharm Technol Res. 2022. PMID: 36568048 Free PMC article.
-
Molecular and Cellular Mechanisms of Perineural Invasion in Oral Squamous Cell Carcinoma: Potential Targets for Therapeutic Intervention.Cancers (Basel). 2021 Nov 29;13(23):6011. doi: 10.3390/cancers13236011. Cancers (Basel). 2021. PMID: 34885121 Free PMC article. Review.
-
Preclinical Assessment of the Effectiveness of Magnetic Resonance Molecular Imaging of Extradomain-B Fibronectin for Detection and Characterization of Oral Cancer.Mol Imaging Biol. 2020 Dec;22(6):1532-1542. doi: 10.1007/s11307-020-01524-6. Epub 2020 Aug 12. Mol Imaging Biol. 2020. PMID: 32789648 Free PMC article.
References
-
- Kordek R, Jassem J, Jeziorski A, et al. Oncology Handbook for students and practitioners. 3rd ed. Gdansk: Via Medica; 2007. pp. 147–58.
-
- Gajecka M, Rydzanic M, Jaskula-Sztul R, et al. Reduced DNA repair capacity in laryngeal cancer subjects. A comparison of phenotypic and genotypic results. Adv Otorhinolaryngol. 2005;62:25–37. - PubMed
-
- Kawecki A. Epithelial neoplasms of the head and neck organs. In: Krzakowski M, Warzocha K, Kawecki A, et al., editors. Guidelines for diagnostic and therapy of malignant tumors in 2013. 1st ed. I. Gdansk: VM Media; 2013. pp. 1–32.
-
- Didkowska J, Wojciechowska U. Malignant tumors in Poland in 2013. Warsaw: National Cancer Registry; 2015. pp. 52–54.pp. 82–84.
-
- Stachura J, Domagała W. Pathology: A word about the disease. 2nd ed. I. Krakow: Polish Academy of Knowledge; 2008. pp. 156–217.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials