

Interleukin 6 Inhibition and Coronary Artery Disease in a High-Risk Population: A Prospective Community-Based Clinical Study
- PMID: 28288972
- PMCID: PMC5524026
- DOI: 10.1161/JAHA.116.005038
Interleukin 6 Inhibition and Coronary Artery Disease in a High-Risk Population: A Prospective Community-Based Clinical Study
Abstract
Background: Atherosclerosis is a chronic inflammatory disease, with interleukin 6 (IL-6) as a major player in inflammation cascade. IL-6 blockade may reduce cardiovascular risk, but current treatments to block IL-6 also induce dyslipidemia, a finding with an uncertain prognosis.
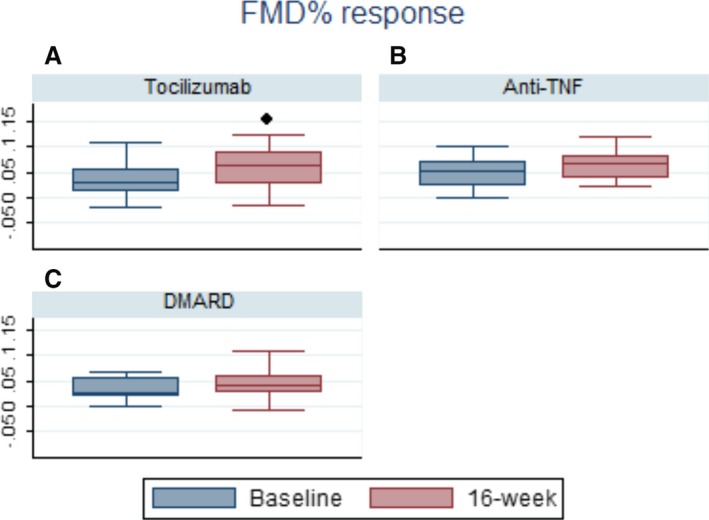
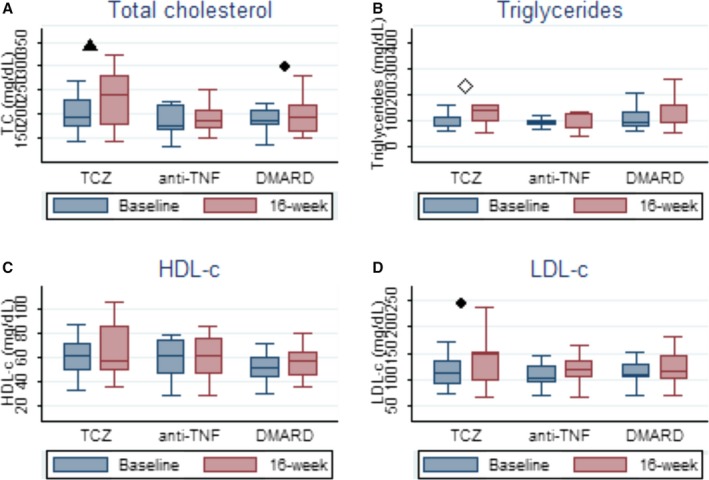
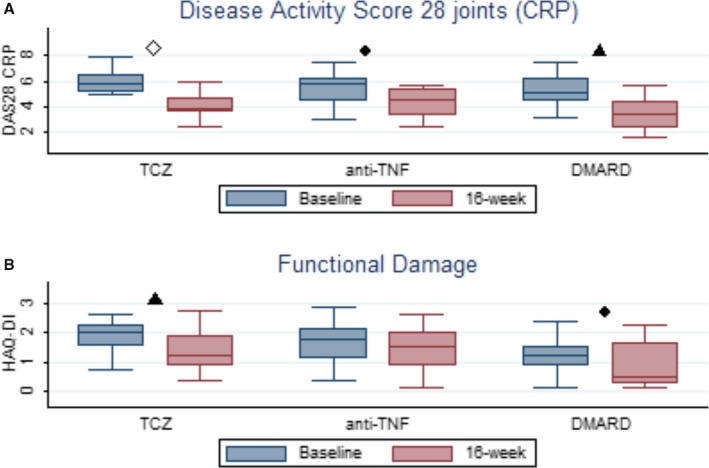
Methods and results: We aimed to determine the endothelial function responses to the IL-6-blocking agent tocilizumab, anti-tumor necrosis factor α, and synthetic disease-modifying antirheumatic drug therapies in patients with rheumatoid arthritis in a 16-week prospective study. Sixty consecutive patients with rheumatoid arthritis were enrolled. Tocilizumab and anti-tumor necrosis factor α therapy were started in 18 patients each while 24 patients were treated with synthetic disease-modifying antirheumatic drugs. Forty patients completed the 16-week follow-up period. The main outcome was flow-mediated dilation percentage variation before and after therapy. In the tocilizumab group, flow-mediated dilation percentage variation increased statistically significantly from a pre-treatment mean of (3.43% [95% CI, 1.28-5.58] to 5.96% [95% CI, 3.95-7.97]; P=0.03). Corresponding changes were 4.78% (95% CI, 2.13-7.42) to 6.75% (95% CI, 4.10-9.39) (P=0.09) and 2.87% (95% CI, -2.17 to 7.91) to 4.84% (95% CI, 2.61-7.07) (P=0.21) in the anti-tumor necrosis factor α and the synthetic disease-modifying antirheumatic drug groups, respectively (both not statistically significant). Total cholesterol increased significantly in the tocilizumab group from 197.5 (95% CI, 177.59-217.36) to 232.3 (201.62-263.09) (P=0.003) and in the synthetic disease-modifying antirheumatic drug group from 185.8 (95% CI, 169.76-201.81) to 202.8 (95% CI, 176.81-228.76) (P=0.04), but not in the anti-tumor necrosis factor α group. High-density lipoprotein did not change significantly in any group.
Conclusions: Endothelial function is improved by tocilizumab in a high-risk population, even as it increases total cholesterol and low-density lipoprotein levels.
Keywords: dyslipidemia; endothelial function; inflammation; tocilizumab.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
Similar articles
-
[The efficacy and safety of tocilizumab combined with disease-modifying anti-rheumatoid drugs in the treatment of active rheumatoid arthritis: a multi-center, randomized, double-blinded, placebo-controlled trial].Zhonghua Nei Ke Za Zhi. 2013 Apr;52(4):323-9. Zhonghua Nei Ke Za Zhi. 2013. PMID: 23925361 Clinical Trial. Chinese.
-
Early rheumatoid arthritis treated with tocilizumab, methotrexate, or their combination (U-Act-Early): a multicentre, randomised, double-blind, double-dummy, strategy trial.Lancet. 2016 Jul 23;388(10042):343-355. doi: 10.1016/S0140-6736(16)30363-4. Epub 2016 Jun 7. Lancet. 2016. PMID: 27287832 Clinical Trial.
-
Interleukin-6 receptor inhibition with tocilizumab reduces disease activity in rheumatoid arthritis with inadequate response to disease-modifying antirheumatic drugs: the tocilizumab in combination with traditional disease-modifying antirheumatic drug therapy study.Arthritis Rheum. 2008 Oct;58(10):2968-80. doi: 10.1002/art.23940. Arthritis Rheum. 2008. PMID: 18821691 Clinical Trial.
-
Interleukin-6 in rheumatoid arthritis.Curr Opin Rheumatol. 2006 May;18(3):277-81. doi: 10.1097/01.bor.0000218949.19860.d1. Curr Opin Rheumatol. 2006. PMID: 16582692 Review.
-
IL-6 inhibitors for treatment of rheumatoid arthritis: past, present, and future.Arch Pharm Res. 2015;38(5):575-84. doi: 10.1007/s12272-015-0569-8. Epub 2015 Feb 4. Arch Pharm Res. 2015. PMID: 25648633 Review.
Cited by
-
Cardiovascular Disease Risk in Rheumatoid Arthritis Anno 2022.J Clin Med. 2022 May 11;11(10):2704. doi: 10.3390/jcm11102704. J Clin Med. 2022. PMID: 35628831 Free PMC article. Review.
-
Protective Effects of Methotrexate against Proatherosclerotic Cytokines: A Review of the Evidence.Mediators Inflamm. 2017;2017:9632846. doi: 10.1155/2017/9632846. Epub 2017 Dec 21. Mediators Inflamm. 2017. PMID: 29430085 Free PMC article. Review.
-
Effect of a Combination of Citrus Flavones and Flavanones and Olive Polyphenols for the Reduction of Cardiovascular Disease Risk: An Exploratory Randomized, Double-Blind, Placebo-Controlled Study in Healthy Subjects.Nutrients. 2020 May 19;12(5):1475. doi: 10.3390/nu12051475. Nutrients. 2020. PMID: 32438719 Free PMC article. Clinical Trial.
-
Impaired peroxisomal import in Drosophila oenocytes causes cardiac dysfunction by inducing upd3 as a peroxikine.Nat Commun. 2020 Jun 10;11(1):2943. doi: 10.1038/s41467-020-16781-w. Nat Commun. 2020. PMID: 32523050 Free PMC article.
-
Interleukin-6 and the Risk of Adverse Outcomes in Patients After an Acute Coronary Syndrome: Observations From the SOLID-TIMI 52 (Stabilization of Plaque Using Darapladib-Thrombolysis in Myocardial Infarction 52) Trial.J Am Heart Assoc. 2017 Oct 24;6(10):e005637. doi: 10.1161/JAHA.117.005637. J Am Heart Assoc. 2017. PMID: 29066436 Free PMC article.
References
-
- Ross R. Atherosclerosis—an inflammatory disease. N Engl J Med. 1999;340:115–126. - PubMed
-
- Sattar N, McCarey DW, Capell H, McInnes IB. Explaining how “high‐grade” systemic inflammation accelerates vascular risk in rheumatoid arthritis. Circulation. 2003;108:2957–2963. - PubMed
-
- McInnes IB, Thompson L, Giles JT, Bathon JM, Salmon JE, Beaulieu AD, Codding CE, Carlson TH, Delles C, Lee JS, Sattar N. Effect of interleukin‐6 receptor blockade on surrogates of vascular risk in rheumatoid arthritis: MEASURE, a randomised, placebo‐controlled study. Ann Rheum Dis. 2013;1–9. - PMC - PubMed
-
- Ridker PM, Danielson E, Fonseca FAH, Genest J, Gotto AM, Kastelein JJP, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT, Glynn RJ; JUPITER Study Group. Rosuvastatin to prevent vascular events in men and women with elevated C‐reactive protein. N Engl J Med. 2008;359:2195–2207. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
