

Patient Age, Sex, and Inflammatory Bowel Disease Phenotype Associate With Course of Primary Sclerosing Cholangitis
- PMID: 28274849
- PMCID: PMC5546611
- DOI: 10.1053/j.gastro.2017.02.038
Patient Age, Sex, and Inflammatory Bowel Disease Phenotype Associate With Course of Primary Sclerosing Cholangitis
Abstract
Background & aims: Primary sclerosing cholangitis (PSC) is an orphan hepatobiliary disorder associated with inflammatory bowel disease (IBD). We aimed to estimate the risk of disease progression based on distinct clinical phenotypes in a large international cohort of patients with PSC.
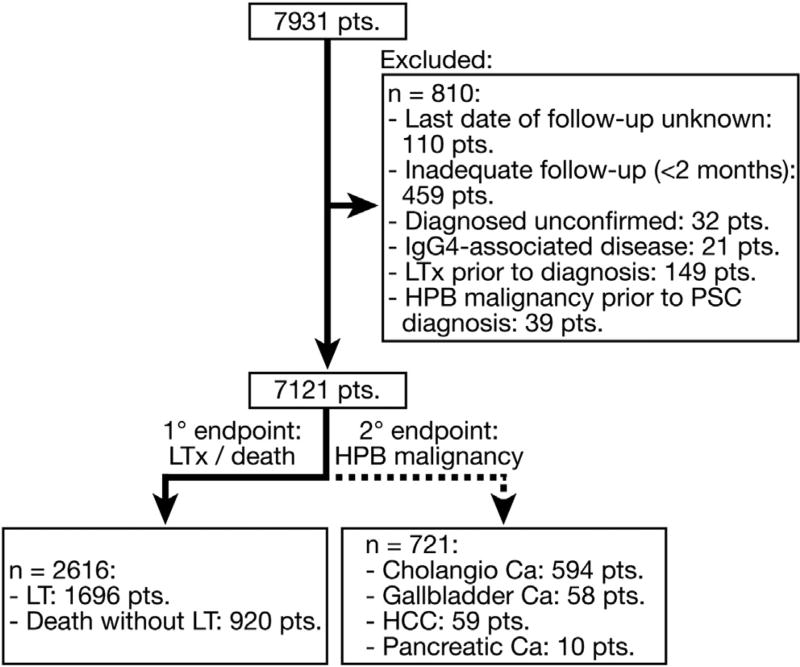
Methods: We performed a retrospective outcome analysis of patients diagnosed with PSC from 1980 through 2010 at 37 centers in Europe, North America, and Australia. For each patient, we collected data on sex, clinician-reported age at and date of PSC and IBD diagnoses, phenotypes of IBD and PSC, and date and indication of IBD-related surgeries. The primary and secondary endpoints were liver transplantation or death (LTD) and hepatopancreatobiliary malignancy, respectively. Cox proportional hazards models were applied to determine the effects of individual covariates on rates of clinical events, with time-to-event analysis ascertained through Kaplan-Meier estimates.
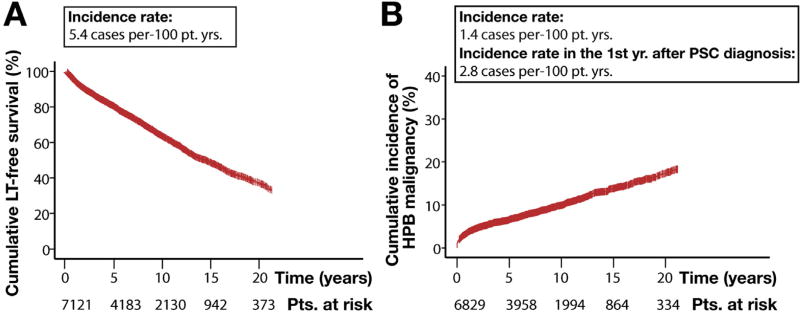
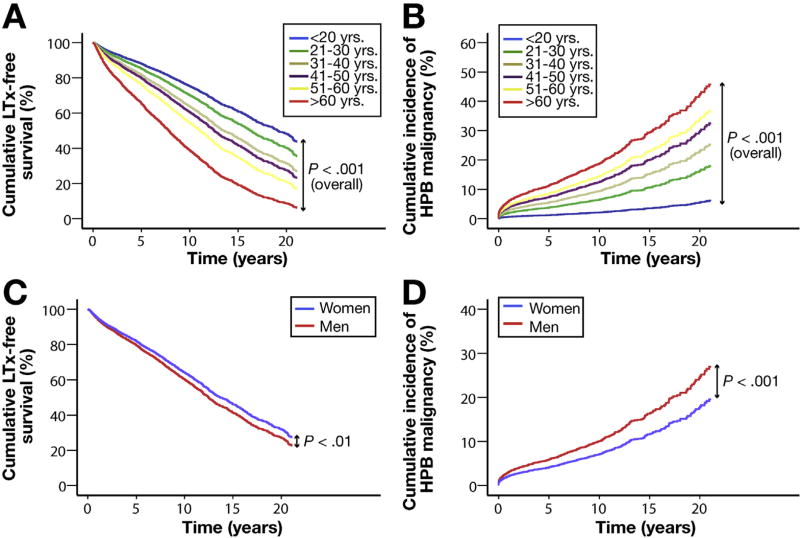
Results: Of the 7121 patients in the cohort, 2616 met the primary endpoint (median time to event of 14.5 years) and 721 developed hepatopancreatobiliary malignancy. The most common malignancy was cholangiocarcinoma (n = 594); patients of advanced age at diagnosis had an increased incidence compared with younger patients (incidence rate: 1.2 per 100 patient-years for patients younger than 20 years old, 6.0 per 100 patient-years for patients 21-30 years old, 9.0 per 100 patient-years for patients 31-40 years old, 14.0 per 100 patient-years for patients 41-50 years old, 15.2 per 100 patient-years for patients 51-60 years old, and 21.0 per 100 patient-years for patients older than 60 years). Of all patients with PSC studied, 65.5% were men, 89.8% had classical or large-duct disease, and 70.0% developed IBD at some point. Assessing the development of IBD as a time-dependent covariate, Crohn's disease and no IBD (both vs ulcerative colitis) were associated with a lower risk of LTD (unadjusted hazard ratio [HR], 0.62; P < .001 and HR, 0.90; P = .03, respectively) and malignancy (HR, 0.68; P = .008 and HR, 0.77; P = .004, respectively). Small-duct PSC was associated with a lower risk of LTD or malignancy compared with classic PSC (HR, 0.30 and HR, 0.15, respectively; both P < .001). Female sex was also associated with a lower risk of LTD or malignancy (HR, 0.88; P = .002 and HR, 0.68; P < .001, respectively). In multivariable analyses assessing the primary endpoint, small-duct PSC characterized a low-risk phenotype in both sexes (adjusted HR for men, 0.23; P < .001 and adjusted HR for women, 0.48; P = .003). Conversely, patients with ulcerative colitis had an increased risk of liver disease progression compared with patients with Crohn's disease (HR, 1.56; P < .001) or no IBD (HR, 1.15; P = .002).
Conclusions: In an analysis of data from individual patients with PSC worldwide, we found significant variation in clinical course associated with age at diagnosis, sex, and ductal and IBD subtypes. The survival estimates provided might be used to estimate risk levels for patients with PSC and select patients for clinical trials.
Keywords: Autoimmune Liver Disease; Cholestasis; Immune-Mediated Liver Disease; Risk Stratification.
Copyright © 2017 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors disclose no conflicts.
Figures

Similar articles
-
Primary sclerosing cholangitis in the Swiss Inflammatory Bowel Disease Cohort Study: prevalence, risk factors, and long-term follow-up.Eur J Gastroenterol Hepatol. 2017 Jan;29(1):91-97. doi: 10.1097/MEG.0000000000000747. Eur J Gastroenterol Hepatol. 2017. PMID: 27622999
-
Patients with large-duct primary sclerosing cholangitis and Crohn's disease have a better outcome than those with ulcerative colitis, or without IBD.Aliment Pharmacol Ther. 2016 Mar;43(5):612-20. doi: 10.1111/apt.13516. Epub 2016 Jan 8. Aliment Pharmacol Ther. 2016. PMID: 26748470
-
Clinical aspects and prognosis of patients with inflammatory bowel disease associated with autoimmune liver diseases.Gastroenterol Hepatol. 2022 Feb;45(2):83-90. doi: 10.1016/j.gastrohep.2021.03.011. Epub 2021 May 20. Gastroenterol Hepatol. 2022. PMID: 34023469 English, Spanish.
-
Primary sclerosing cholangitis associated with inflammatory bowel disease: an update.Eur J Gastroenterol Hepatol. 2016 Feb;28(2):123-31. doi: 10.1097/MEG.0000000000000532. Eur J Gastroenterol Hepatol. 2016. PMID: 26636407 Review.
-
Distinctive inflammatory bowel disease phenotype in primary sclerosing cholangitis.World J Gastroenterol. 2015 Feb 14;21(6):1956-71. doi: 10.3748/wjg.v21.i6.1956. World J Gastroenterol. 2015. PMID: 25684965 Free PMC article. Review.
Cited by
-
African American race does not confer an increased risk of clinical events in patients with primary sclerosing cholangitis.Hepatol Commun. 2024 Jan 29;8(2):e0366. doi: 10.1097/HC9.0000000000000366. eCollection 2024 Feb 1. Hepatol Commun. 2024. PMID: 38285883 Free PMC article.
-
Geoepidemiologic variation in outcomes of primary sclerosing cholangitis.World J Hepatol. 2020 Apr 27;12(4):116-124. doi: 10.4254/wjh.v12.i4.116. World J Hepatol. 2020. PMID: 32685104 Free PMC article. Review.
-
Surrogate markers of bile duct disease progression in primary sclerosing cholangitis - A prospective study with repeated ERCP examinations.JHEP Rep. 2024 Jul 2;6(10):101161. doi: 10.1016/j.jhepr.2024.101161. eCollection 2024 Oct. JHEP Rep. 2024. PMID: 39290402 Free PMC article.
-
Risk of hepato-pancreato-biliary cancer is increased by primary sclerosing cholangitis in patients with inflammatory bowel disease: A population-based cohort study.United European Gastroenterol J. 2022 Mar;10(2):212-224. doi: 10.1002/ueg2.12204. Epub 2022 Feb 2. United European Gastroenterol J. 2022. PMID: 35107865 Free PMC article.
-
The clinical significance of biliary findings in magnetic resonance enterography of patients with inflammatory bowel disease.Pol J Radiol. 2022 Nov 12;87:e613-e621. doi: 10.5114/pjr.2022.121443. eCollection 2022. Pol J Radiol. 2022. PMID: 36532253 Free PMC article.
References
-
- Hirschfield GM, Karlsen TH, Lindor KD, Adams DH. Primary sclerosing cholangitis. Lancet. 2013;382:1587–1599. - PubMed
-
- Boonstra K, Weersma RK, van Erpecum KJ, et al. Population-based epidemiology, malignancy risk, and outcome of primary sclerosing cholangitis. Hepatology. 2013;58:2045–2055. - PubMed
-
- Boonstra K, Beuers U, Ponsioen CY. Epidemiology of primary sclerosing cholangitis and primary biliary cirrhosis: a systematic review. J Hepatol. 2012;56:1181–1188. - PubMed
-
- Lindkvist B, Benito de Valle M, Gullberg B, Björnsson E. Incidence and prevalence of primary sclerosing cholangitis in a defined adult population in Sweden. Hepatology. 2010;52:571–577. - PubMed
-
- Patkowski W, Skalski M, Zieniewicz K, et al. Orthotopic liver transplantation for cholestatic diseases. Hepatogastroenterology. 2010;57:605–610. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
