

Acute-on-chronic liver failure: an update
- PMID: 28053053
- PMCID: PMC5534763
- DOI: 10.1136/gutjnl-2016-312670
Acute-on-chronic liver failure: an update
Abstract
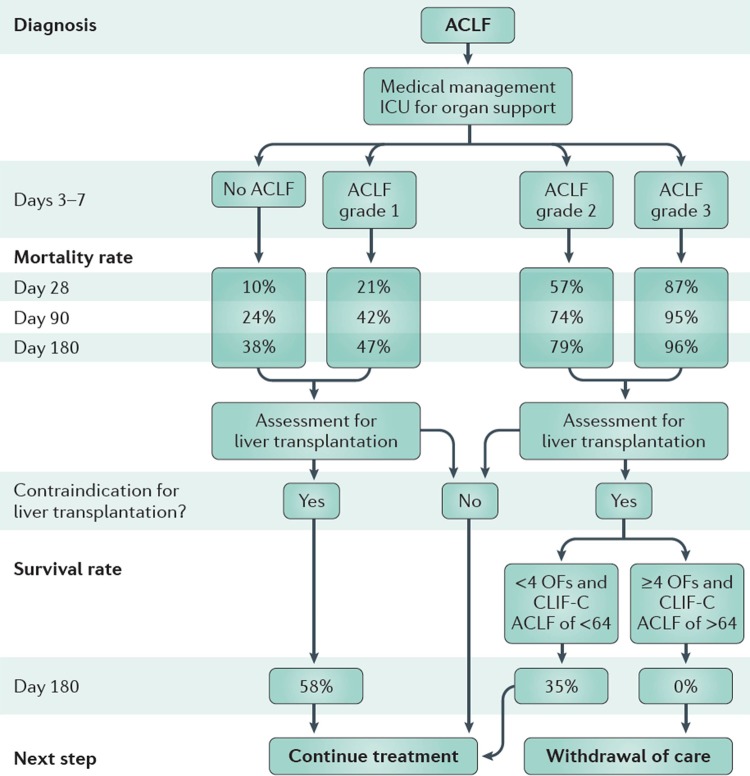
Acute-on-chronic liver failure (ACLF) is a syndrome characterised by acute decompensation of chronic liver disease associated with organ failures and high short-term mortality. Alcohol and chronic viral hepatitis are the most common underlying liver diseases. Up to 40%-50% of the cases of ACLF have no identifiable trigger; in the remaining patients, sepsis, active alcoholism and relapse of chronic viral hepatitis are the most common reported precipitating factors. An excessive systemic inflammatory response seems to play a crucial role in the development of ACLF. Using a liver-adapted sequential organ assessment failure score, it is possible to triage and prognosticate the outcome of patients with ACLF. The course of ACLF is dynamic and changes over the course of hospital admission. Most of the patients will have a clear prognosis between day 3 and 7 of hospital admission and clinical decisions such as evaluation for liver transplant or discussion over goals of care could be tailored using clinical scores. Bioartificial liver support systems, granulocyte-colony stimulating factors or stem-cell transplant are in the horizon of medical care of this patient population; however, data are too premature to implement them as standard of care.
Keywords: LIVER CIRRHOSIS; LIVER FAILURE.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Figures
Comment in
-
Acute-on-chronic liver failure-old concepts made clearer.Transl Gastroenterol Hepatol. 2017 Dec 18;2:111. doi: 10.21037/tgh.2017.11.17. eCollection 2017. Transl Gastroenterol Hepatol. 2017. PMID: 29354768 Free PMC article. No abstract available.
Similar articles
-
Update on acute-on-chronic liver failure.Gastroenterol Hepatol. 2018 Jan;41(1):43-53. doi: 10.1016/j.gastrohep.2017.05.012. Epub 2017 Jun 24. Gastroenterol Hepatol. 2018. PMID: 28655410 Review. English, Spanish.
-
Acute-on-chronic liver failure in cirrhosis.Nat Rev Dis Primers. 2016 Jun 9;2:16041. doi: 10.1038/nrdp.2016.41. Nat Rev Dis Primers. 2016. PMID: 27277335 Review.
-
Acute-on-chronic liver failure: A new syndrome that will re-classify cirrhosis.J Hepatol. 2015 Apr;62(1 Suppl):S131-43. doi: 10.1016/j.jhep.2014.11.045. J Hepatol. 2015. PMID: 25920082 Review.
-
PREDICT identifies precipitating events associated with the clinical course of acutely decompensated cirrhosis.J Hepatol. 2021 May;74(5):1097-1108. doi: 10.1016/j.jhep.2020.11.019. Epub 2020 Nov 20. J Hepatol. 2021. PMID: 33227350
-
Acute-on-chronic liver failure: a new clinical entity.Clin Gastroenterol Hepatol. 2015 May;13(5):836-41. doi: 10.1016/j.cgh.2014.02.027. Epub 2014 Feb 28. Clin Gastroenterol Hepatol. 2015. PMID: 24583872
Cited by
-
Effect of COVID-19 on patients with compensated chronic liver diseases.Hepatol Int. 2020 Sep;14(5):701-710. doi: 10.1007/s12072-020-10058-6. Epub 2020 Jul 30. Hepatol Int. 2020. PMID: 32734407 Free PMC article.
-
Galectin-3 critically mediates the hepatoprotection conferred by M2-like macrophages in ACLF by inhibiting pyroptosis but not necroptosis signalling.Cell Death Dis. 2022 Sep 8;13(9):775. doi: 10.1038/s41419-022-05181-1. Cell Death Dis. 2022. PMID: 36075893 Free PMC article.
-
Sorafenib-induced Acute on Chronic Liver Failure in a Patient with Hepatocellular Carcinoma After Microwave Ablation.Cureus. 2019 Jul 19;11(7):e5176. doi: 10.7759/cureus.5176. Cureus. 2019. PMID: 31565587 Free PMC article.
-
Prognosis prediction performs better in patients with non-cirrhosis hepatitis B virus-related acute-on-chronic liver failure than those with cirrhosis.Front Microbiol. 2022 Dec 9;13:1013439. doi: 10.3389/fmicb.2022.1013439. eCollection 2022. Front Microbiol. 2022. PMID: 36569093 Free PMC article.
-
Animal models applied to acute-on-chronic liver failure: Are new models required to understand the human condition?World J Clin Cases. 2022 Mar 26;10(9):2687-2699. doi: 10.12998/wjcc.v10.i9.2687. World J Clin Cases. 2022. PMID: 35434112 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources