

Rovalpituzumab tesirine, a DLL3-targeted antibody-drug conjugate, in recurrent small-cell lung cancer: a first-in-human, first-in-class, open-label, phase 1 study
- PMID: 27932068
- PMCID: PMC5481162
- DOI: 10.1016/S1470-2045(16)30565-4
Rovalpituzumab tesirine, a DLL3-targeted antibody-drug conjugate, in recurrent small-cell lung cancer: a first-in-human, first-in-class, open-label, phase 1 study
Abstract
Background: Rovalpituzumab tesirine is a first-in-class antibody-drug conjugate directed against delta-like protein 3 (DLL3), a novel target identified in tumour-initiating cells and expressed in more than 80% of patients with small-cell lung cancer. We aimed to assess the safety and activity of rovalpituzumab tesirine in patients who progressed after one or more previous regimen.
Methods: We conducted a phase 1 open-label study at ten cancer centres in the USA. Eligible patients were aged 18 years or older and had histologically or cytologically confirmed small-cell lung cancer or large-cell neuroendocrine tumours with progressive measurable disease (according to Response Evaluation Criteria in Solid Tumors [RECIST], version 1.1) previously treated with one or two chemotherapeutic regimens, including a platinum-based regimen. We assigned patients to dose-escalation or expansion cohorts, ranging from 0·05 mg/kg to 0·8 mg/kg rovalpituzumab tesirine intravenously every 3 weeks or every 6 weeks, followed by investigation of the dose schedules 0·3 mg/kg and 0·4 mg/kg every 6 weeks and 0·2 mg/kg every 3 weeks. Primary objectives were to assess the safety of rovalpituzumab tesirine, including the maximum tolerated dose and dose-limiting toxic effects. The primary activity endpoint was objective response by intention-to-treat analysis. This study is registered with ClinicalTrials.gov, number NCT01901653. The study is closed to enrolment; this report focuses on the cohort with small-cell lung cancer.
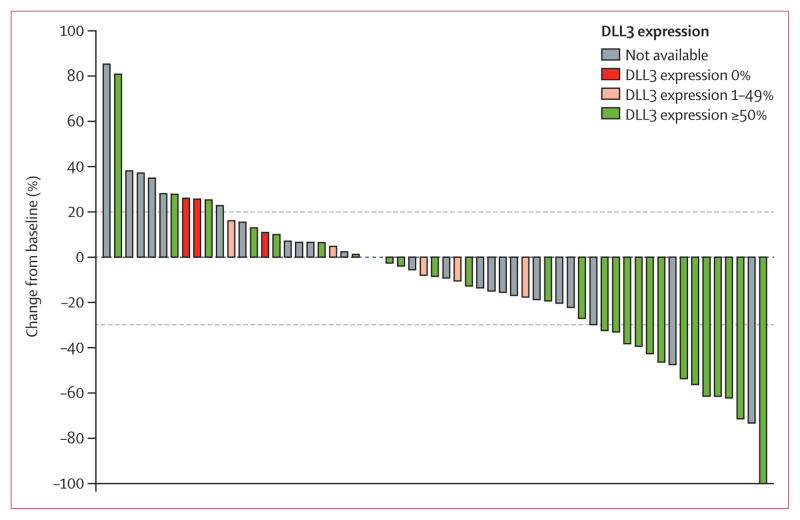
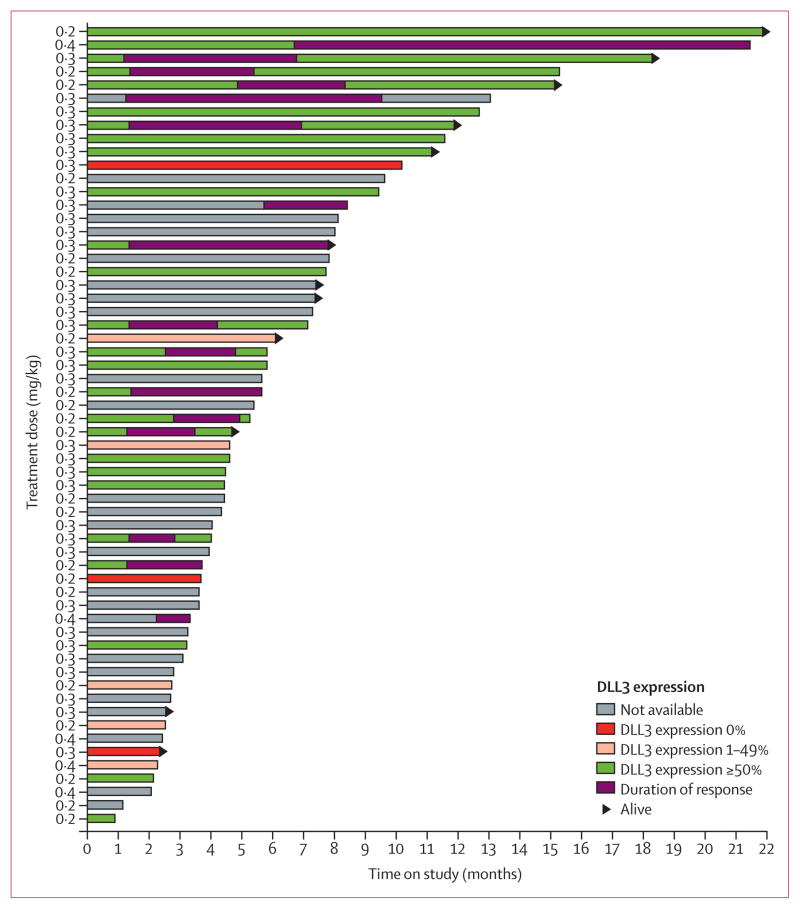
Findings: Between July 22, 2013, and Aug 10, 2015, 82 patients were enrolled, including 74 patients with small-cell lung cancer and eight with large-cell neuroendocrine carcinoma, all of whom received at least one dose of rovalpituzumab tesirine. Dose-limiting toxic effects of rovalpituzumab tesirine occurred at a dose of 0·8 mg/kg every 3 weeks, including grade 4 thrombocytopenia (in two of two patients at that dose level) and grade 4 liver function test abnormalities (in one patient). The most frequent grade 3 or worse treatment-related adverse events in 74 patients with small-cell lung cancer were thrombocytopenia (eight [11%]), pleural effusion (six [8%]), and increased lipase (five [7%]). Drug-related serious adverse events occurred in 28 (38%) of 74 patients. The maximum tolerated dose of rovalpituzumab tesirine was 0·4 mg/kg every 3 weeks; the recommended phase 2 dose and schedule is 0·3 mg/kg every 6 weeks. At active doses of rovalpituzumab tesirine (0·2 mg/kg or 0·4 mg/kg every 3 weeks or 0·3 mg/kg or 0·4 mg/kg every 6 weeks), 11 (18%) of 60 assessable patients had a confirmed objective response. 11 (18%) of 60 assessable patients had a confirmed objective response, including ten (38%) of 26 patients confirmed to have high DLL3 expression (expression in 50% or more of tumour cells).
Interpretation: Rovalpituzumab tesirine shows encouraging single-agent antitumour activity with a manageable safety profile. Further development of rovalpituzumab tesirine in DLL3-expressing malignant diseases is warranted.
Funding: Stemcentrx Inc.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
CMR reports consulting fees from Bristol-Myers Squibb, Medivation, and Novartis, outside the published work. MCP reports consulting fees from Celgene, Abbvie, Clovis, Novartis, and Bristol-Myers Squibb; and is currently employed by Merck Research Laboratories, outside the submitted work. DMo reports personal fees from Celgene, Heat Biologics, Bristol-Myers Squibb, and Genentech for advisory board membership, and from Boehringer Ingelheim and Genentech for speakers bureau attendance, outside the submitted work. BSG reports clinical trial contracts with Amgen, Oncomed, and MedImmune, and trial support from Bristol-Myers Squibb and ISA Pharmaceuticals, outside the submitted report. LAB reports consulting fees from Biomarin, AstraZeneca, and Abbvie, outside the submitted work. FR reports personal fees for speakers bureau attendance from Boehringer Ingelheim and Merck, outside the submitted work. RG reports personal fees for consulting or honoraria from GlaxoSmithKline, Celgene, Roche, Bayer, Genentech, Clovis, Helsinn Healthcare, Baxalta, Pfizer, Astellas, and ARIAD, outside the submitted work. THH, SB, HZ, SL, SJD, and SLP were employees of Stemcentrx during the conduct of this study. THH is a shareholder in Stemcentrx and has a patent pending for use of DLL3 antibody-drug conjugates. SJD is a shareholder in Stemcentrx and has several patents issued that are relevant to the current work: USPN 9,089,617; USPN 9,173,959; USPN 9,352,091; USPN 9,358,304; USPN 9,089,616; USPN 9,133,271; USPN 9,155,803; and USPN 9,345,784. NT, SW, DMa, and BV were employees of Ventana Medical Systems during the conduct of this study. TMB, NR, MLJ, HAB, DKS, and DRS declare no competing interests.
Figures
Comment in
-
Rovalpituzumab tesirine and DLL3: a new challenge for small-cell lung cancer.Lancet Oncol. 2017 Jan;18(1):3-5. doi: 10.1016/S1470-2045(16)30575-7. Epub 2016 Dec 5. Lancet Oncol. 2017. PMID: 27932065 No abstract available.
Similar articles
-
Efficacy and Safety of Rovalpituzumab Tesirine in Third-Line and Beyond Patients with DLL3-Expressing, Relapsed/Refractory Small-Cell Lung Cancer: Results From the Phase II TRINITY Study.Clin Cancer Res. 2019 Dec 1;25(23):6958-6966. doi: 10.1158/1078-0432.CCR-19-1133. Epub 2019 Sep 10. Clin Cancer Res. 2019. PMID: 31506387 Free PMC article. Clinical Trial.
-
Phase I safety and pharmacokinetics study of rovalpituzumab tesirine in Japanese patients with advanced, recurrent small cell lung cancer.Lung Cancer. 2019 Sep;135:145-150. doi: 10.1016/j.lungcan.2019.07.025. Epub 2019 Jul 24. Lung Cancer. 2019. PMID: 31446987 Clinical Trial.
-
Prevalence of Delta-like protein 3 expression in patients with small cell lung cancer.Lung Cancer. 2018 Jan;115:116-120. doi: 10.1016/j.lungcan.2017.11.018. Epub 2017 Nov 22. Lung Cancer. 2018. PMID: 29290251
-
DLL3: an emerging target in small cell lung cancer.J Hematol Oncol. 2019 Jun 18;12(1):61. doi: 10.1186/s13045-019-0745-2. J Hematol Oncol. 2019. PMID: 31215500 Free PMC article. Review.
-
Rovalpituzumab Tesirine: A Novel DLL3-Targeting Antibody-Drug Conjugate.Drugs R D. 2018 Dec;18(4):255-258. doi: 10.1007/s40268-018-0247-7. Drugs R D. 2018. PMID: 30232719 Free PMC article. Review.
Cited by
-
Efficacy and toxicity of lurbinectedin in subsequent systemic therapy of extensive-stage small cell lung cancer: a meta-analysis.BMC Cancer. 2024 Nov 4;24(1):1351. doi: 10.1186/s12885-024-13104-w. BMC Cancer. 2024. PMID: 39497053 Free PMC article.
-
Advancing Treatment Options for Merkel Cell Carcinoma: A Review of Tumor-Targeted Therapies.Int J Mol Sci. 2024 Oct 15;25(20):11055. doi: 10.3390/ijms252011055. Int J Mol Sci. 2024. PMID: 39456853 Free PMC article. Review.
-
Vesiculobullous eruption with loncastuximab tesirine in a patient with relapsed follicular lymphoma.JAAD Case Rep. 2024 Sep 2;53:1-5. doi: 10.1016/j.jdcr.2024.08.013. eCollection 2024 Nov. JAAD Case Rep. 2024. PMID: 39421259 Free PMC article. No abstract available.
-
Activating Invasion and Metastasis in Small Cell Lung Cancer: Role of the Tumour Immune Microenvironment and Mechanisms of Vasculogenesis, Epithelial-Mesenchymal Transition, Cell Migration, and Organ Tropism.Cancer Rep (Hoboken). 2024 Oct;7(10):e70018. doi: 10.1002/cnr2.70018. Cancer Rep (Hoboken). 2024. PMID: 39376011 Free PMC article. Review.
-
Neuroendocrine transdifferentiation in human cancer: molecular mechanisms and therapeutic targets.MedComm (2020). 2024 Oct 4;5(10):e761. doi: 10.1002/mco2.761. eCollection 2024 Oct. MedComm (2020). 2024. PMID: 39372390 Free PMC article. Review.
References
-
- Ferlay J, Soerjomataram I, Ervik M, et al. [accessed April 4, 2016];GLOBOCAN 2012 version 1.0: cancer incidence and mortality worldwide—IARC CancerBase no 11. 2013 http://globocan.iarc.fr.
-
- Fruh M, De Ruysscher D, Popat S, et al. Small-cell lung cancer (SCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(suppl 6):vi99–105. - PubMed
-
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: small cell lung cancer, version 2. Fort Washington: National Comprehensive Cancer Network; 2016.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
