

Skeletal muscle quality as assessed by CT-derived skeletal muscle density is associated with 6-month mortality in mechanically ventilated critically ill patients
- PMID: 27903267
- PMCID: PMC5131531
- DOI: 10.1186/s13054-016-1563-3
Skeletal muscle quality as assessed by CT-derived skeletal muscle density is associated with 6-month mortality in mechanically ventilated critically ill patients
Abstract
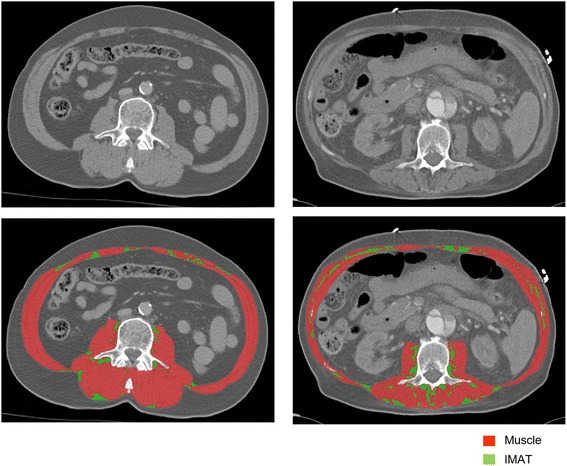
Background: Muscle quantity at intensive care unit (ICU) admission has been independently associated with mortality. In addition to quantity, muscle quality may be important for survival. Muscle quality is influenced by fatty infiltration or myosteatosis, which can be assessed on computed tomography (CT) scans by analysing skeletal muscle density (SMD) and the amount of intermuscular adipose tissue (IMAT). We investigated whether CT-derived low skeletal muscle quality at ICU admission is independently associated with 6-month mortality and other clinical outcomes.
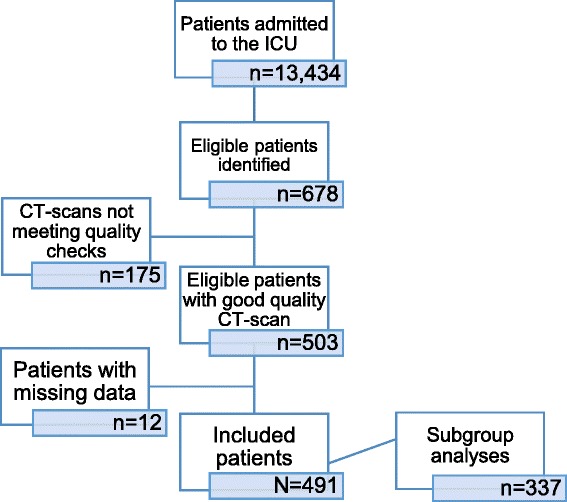
Methods: This retrospective study included 491 mechanically ventilated critically ill adult patients with a CT scan of the abdomen made 1 day before to 4 days after ICU admission. Cox regression analysis was used to determine the association between SMD or IMAT and 6-month mortality, with adjustments for Acute Physiological, Age, and Chronic Health Evaluation (APACHE) II score, body mass index (BMI), and skeletal muscle area. Logistic and linear regression analyses were used for other clinical outcomes.
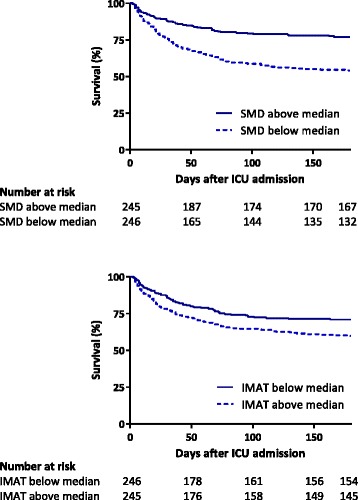
Results: Mean APACHE II score was 24 ± 8 and 6-month mortality was 35.6%. Non-survivors had a lower SMD (25.1 vs. 31.4 Hounsfield Units (HU); p < 0.001), and more IMAT (17.1 vs. 13.3 cm2; p = 0.004). Higher SMD was associated with a lower 6-month mortality (hazard ratio (HR) per 10 HU, 0.640; 95% confidence interval (CI), 0.552-0.742; p < 0.001), and also after correction for APACHE II score, BMI, and skeletal muscle area (HR, 0.774; 95% CI, 0.643-0.931; p = 0.006). Higher IMAT was not significantly associated with higher 6-month mortality after adjustment for confounders. A 10 HU increase in SMD was associated with a 14% shorter hospital length of stay.
Conclusions: Low skeletal muscle quality at ICU admission, as assessed by CT-derived skeletal muscle density, is independently associated with higher 6-month mortality in mechanically ventilated patients. Thus, muscle quality as well as muscle quantity are prognostic factors in the ICU.
Trial registration: Retrospectively registered (initial release on 06/23/2016) at ClinicalTrials.gov: NCT02817646 .
Keywords: CT; Computed tomography; Intensive care unit; Intermuscular adipose tissue; Mortality; Muscle; Muscle quality; Myosteatosis; Outcome; Skeletal muscle density.
Figures
Similar articles
-
Low skeletal muscle area is a risk factor for mortality in mechanically ventilated critically ill patients.Crit Care. 2014 Jan 13;18(2):R12. doi: 10.1186/cc13189. Crit Care. 2014. PMID: 24410863 Free PMC article.
-
Early high protein intake and mortality in critically ill ICU patients with low skeletal muscle area and -density.Clin Nutr. 2020 Jul;39(7):2192-2201. doi: 10.1016/j.clnu.2019.09.007. Epub 2019 Sep 23. Clin Nutr. 2020. PMID: 31669003
-
Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit.JAMA. 2004 Apr 14;291(14):1753-62. doi: 10.1001/jama.291.14.1753. JAMA. 2004. PMID: 15082703
-
Dysphagia in the intensive care unit: epidemiology, mechanisms, and clinical management.Crit Care. 2019 Mar 28;23(1):103. doi: 10.1186/s13054-019-2400-2. Crit Care. 2019. PMID: 30922363 Free PMC article. Review.
-
Measurement of skeletal muscle radiation attenuation and basis of its biological variation.Acta Physiol (Oxf). 2014 Mar;210(3):489-97. doi: 10.1111/apha.12224. Acta Physiol (Oxf). 2014. PMID: 24393306 Free PMC article. Review.
Cited by
-
Modifications of Chest CT Body Composition Parameters at Three and Six Months after Severe COVID-19 Pneumonia: A Retrospective Cohort Study.Nutrients. 2022 Sep 13;14(18):3764. doi: 10.3390/nu14183764. Nutrients. 2022. PMID: 36145141 Free PMC article.
-
Novel approaches to metabolic assessment and structured exercise to promote recovery in ICU survivors.Curr Opin Crit Care. 2020 Aug;26(4):369-378. doi: 10.1097/MCC.0000000000000748. Curr Opin Crit Care. 2020. PMID: 32568800 Free PMC article. Review.
-
The effect of computed tomography parameters on sarcopenia and myosteatosis assessment: a scoping review.J Cachexia Sarcopenia Muscle. 2022 Dec;13(6):2807-2819. doi: 10.1002/jcsm.13068. Epub 2022 Sep 5. J Cachexia Sarcopenia Muscle. 2022. PMID: 36065509 Free PMC article.
-
Evaluation of a Fully Automatic Deep Learning-Based Method for the Measurement of Psoas Muscle Area.Front Nutr. 2022 May 12;9:781860. doi: 10.3389/fnut.2022.781860. eCollection 2022. Front Nutr. 2022. PMID: 35634380 Free PMC article.
-
Skeletal muscle mass and adipose tissue alteration in critically ill patients.PLoS One. 2019 Jun 13;14(6):e0216991. doi: 10.1371/journal.pone.0216991. eCollection 2019. PLoS One. 2019. PMID: 31194755 Free PMC article.
References
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
