

The Latent Reservoir for HIV-1: How Immunologic Memory and Clonal Expansion Contribute to HIV-1 Persistence
- PMID: 27382129
- PMCID: PMC4936486
- DOI: 10.4049/jimmunol.1600343
The Latent Reservoir for HIV-1: How Immunologic Memory and Clonal Expansion Contribute to HIV-1 Persistence
Abstract
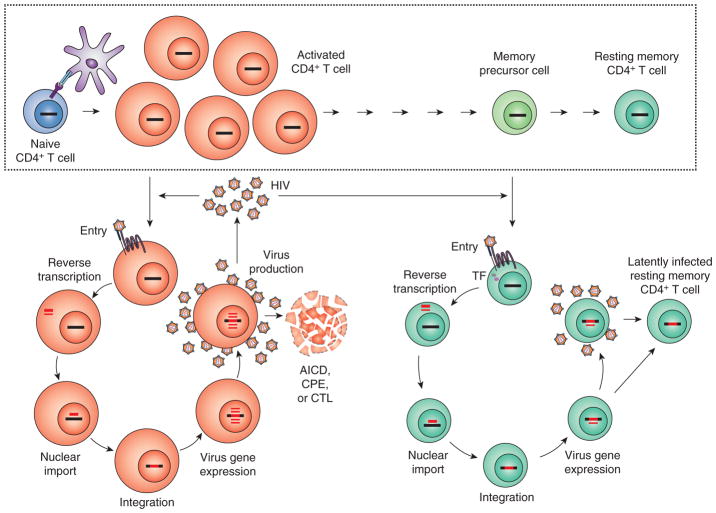
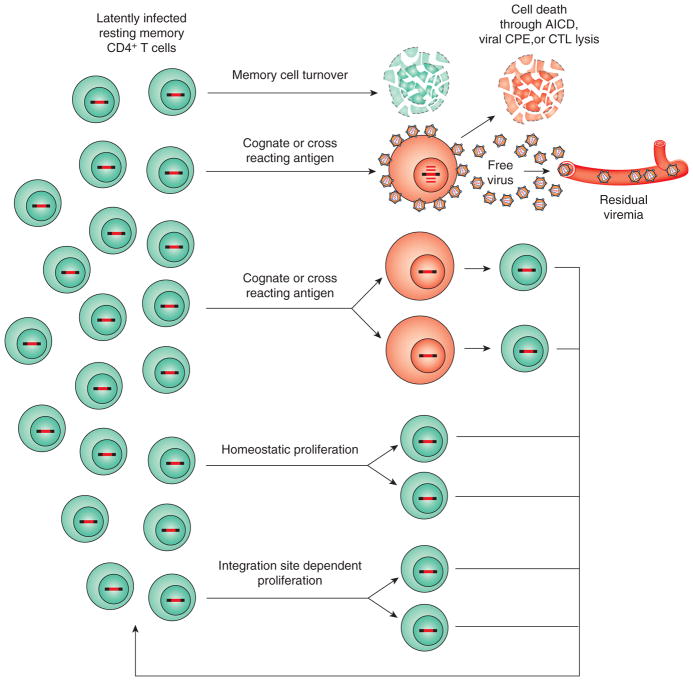
Combination antiretroviral therapy (ART) for HIV-1 infection reduces plasma virus levels to below the limit of detection of clinical assays. However, even with prolonged suppression of viral replication with ART, viremia rebounds rapidly after treatment interruption. Thus, ART is not curative. The principal barrier to cure is a remarkably stable reservoir of latent HIV-1 in resting memory CD4(+) T cells. In this review, we consider explanations for the remarkable stability of the latent reservoir. Stability does not appear to reflect replenishment from new infection events but rather normal physiologic processes that provide for immunologic memory. Of particular importance are proliferative processes that drive clonal expansion of infected cells. Recent evidence suggests that in some infected cells, proliferation is a consequence of proviral integration into host genes associated with cell growth. Efforts to cure HIV-1 infection by targeting the latent reservoir may need to consider the potential of latently infected cells to proliferate.
Copyright © 2016 by The American Association of Immunologists, Inc.
Figures
Similar articles
-
Stable Phenotypic Changes of the Host T Cells Are Essential to the Long-Term Stability of Latent HIV-1 Infection.J Virol. 2015 Jul;89(13):6656-72. doi: 10.1128/JVI.00571-15. Epub 2015 Apr 15. J Virol. 2015. PMID: 25878110 Free PMC article.
-
Effector memory differentiation increases detection of replication-competent HIV-l in resting CD4+ T cells from virally suppressed individuals.PLoS Pathog. 2019 Oct 14;15(10):e1008074. doi: 10.1371/journal.ppat.1008074. eCollection 2019 Oct. PLoS Pathog. 2019. PMID: 31609991 Free PMC article.
-
The forces driving clonal expansion of the HIV-1 latent reservoir.Virol J. 2020 Jan 7;17(1):4. doi: 10.1186/s12985-019-1276-8. Virol J. 2020. PMID: 31910871 Free PMC article. Review.
-
Targeting the Latent Reservoir for HIV-1.Immunity. 2018 May 15;48(5):872-895. doi: 10.1016/j.immuni.2018.04.030. Immunity. 2018. PMID: 29768175 Free PMC article. Review.
-
Phenotypic analysis of the unstimulated in vivo HIV CD4 T cell reservoir.Elife. 2020 Sep 29;9:e60933. doi: 10.7554/eLife.60933. Elife. 2020. PMID: 32990219 Free PMC article.
Cited by
-
Dendritic Cells in HIV/SIV Prophylactic and Therapeutic Vaccination.Viruses. 2019 Dec 24;12(1):24. doi: 10.3390/v12010024. Viruses. 2019. PMID: 31878130 Free PMC article. Review.
-
A Tat/Rev Induced Limiting Dilution Assay to Measure Viral Reservoirs in Non-Human Primate Models of HIV Infection.Sci Rep. 2019 Aug 19;9(1):12078. doi: 10.1038/s41598-019-48354-3. Sci Rep. 2019. PMID: 31427605 Free PMC article.
-
Pitfalls of Antiretroviral Therapy: Current Status and Long-Term CNS Toxicity.Biomolecules. 2022 Jun 26;12(7):894. doi: 10.3390/biom12070894. Biomolecules. 2022. PMID: 35883450 Free PMC article. Review.
-
Impact of LEDGIN treatment during virus production on residual HIV-1 transcription.Retrovirology. 2019 Apr 2;16(1):8. doi: 10.1186/s12977-019-0472-3. Retrovirology. 2019. PMID: 30940165 Free PMC article.
-
Dynamics and mechanisms of clonal expansion of HIV-1-infected cells in a humanized mouse model.Sci Rep. 2017 Jul 31;7(1):6913. doi: 10.1038/s41598-017-07307-4. Sci Rep. 2017. PMID: 28761140 Free PMC article.
References
-
- INSIGHT START Study Group. Lundgren JD, Babiker AG, Gordin F, Emery S, Grund B, Sharma S, Avihingsanon A, Cooper DA, Fatkenheuer G, Llibre JM, Molina JM, Munderi P, Schechter M, Wood R, Klingman KL, Collins S, Lane HC, Phillips AN, Neaton JD. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N Engl J Med. 2015;373:795–807. - PMC - PubMed
-
- Danel C, Moh R, Gabillard D, Badje A, Le Carrou J, Ouassa T, Ouattara E, Anzian A, Ntakpe JB, Minga A, Kouame GM, Bouhoussou F, Emieme A, Kouame A, Inwoley A, Toni TD, Ahiboh H, Kabran M, Rabe C, Sidibe B, Nzunetu G, Konan R, Gnokoro J, Gouesse P, Messou E, Dohoun L, Kamagate S, Yao A, Amon S, Kouame AB, Koua A, Kouame E, Ndri Y, Ba-Gomis O, Daligou M, Ackoundze S, Hawerlander D, Ani A, Dembele F, Kone F, Guehi C, Kanga C, Koule S, Seri J, Oyebi M, Mbakop N, Makaila O, Babatunde C, Babatounde N, Bleoue G, Tchoutedjem M, Kouadio AC, Sena G, Yededji SY, Assi R, Bakayoko A, Mahassadi A, Attia A, Oussou A, Mobio M, Bamba D, Koman M, Horo A, Deschamps N, Chenal H, Sassan-Morokro M, Konate S, Aka K, Aoussi E, Journot V, Nchot C, Karcher S, Chaix ML, Rouzioux C, Sow PS, Perronne C, Girard PM, Menan H, Bissagnene E, Kadio A, Ettiegne-Traore V, Moh-Semde C, Kouame A, Massumbuko JM, Chene G, Dosso M, Domoua SK, N’Dri-Yoman T, Salamon R, Eholie SP, Anglaret X TEMPRANO ANRS 12136 Study Group. A Trial of Early Antiretrovirals and Isoniazid Preventive Therapy in Africa. N Engl J Med. 2015;373:808–822. - PubMed
-
- Gunthard HF, Aberg JA, Eron JJ, Hoy JF, Telenti A, Benson CA, Burger DM, Cahn P, Gallant JE, Glesby MJ, Reiss P, Saag MS, Thomas DL, Jacobsen DM, Volberding PA International Antiviral Society- USA Panel. Antiretroviral treatment of adult HIV infection: 2014 recommendations of the International Antiviral Society-USA Panel. JAMA. 2014;312:410–425. - PubMed
-
- Gulick RM, Mellors JW, Havlir D, Eron JJ, Gonzalez C, McMahon D, Richman DD, Valentine FT, Jonas L, Meibohm A, Emini EA, Chodakewitz JA. Treatment with indinavir, zidovudine, and lamivudine in adults with human immunodeficiency virus infection and prior antiretroviral therapy. N Engl J Med. 1997;337:734–739. - PubMed
-
- Hammer SM, Squires KE, Hughes MD, Grimes JM, Demeter LM, Currier JS, Eron JJ, Jr, Feinberg JE, Balfour HH, Jr, Deyton LR, Chodakewitz JA, Fischl MA. A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency virus infection and CD4 cell counts of 200 per cubic millimeter or less. AIDS Clinical Trials Group 320 Study Team. N Engl J Med. 1997;337:725–733. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials