

Immune checkpoint inhibitor combinations in solid tumors: opportunities and challenges
- PMID: 27349981
- PMCID: PMC5619130
- DOI: 10.2217/imt-2016-0002
Immune checkpoint inhibitor combinations in solid tumors: opportunities and challenges
Abstract
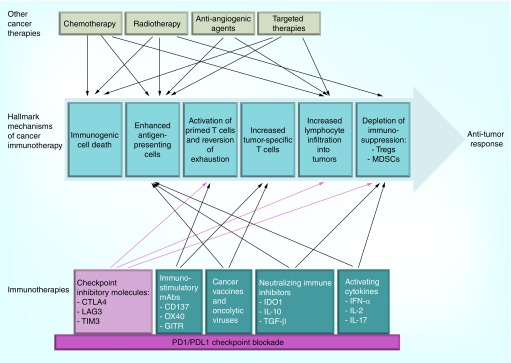
The emergence of immune 'checkpoint inhibitors' such as cytotoxic T-lymphocyte antigen 4 (CTLA-4) and programmed death receptor 1 (PD-1) has revolutionized treatment of solid tumors including melanoma, lung cancer, among many others. The goal of checkpoint inhibitor combination therapy is to improve clinical response and minimize toxicities. Rational design of checkpoint combinations considers immune-mediated mechanisms of antitumor activity: immunogenic cell death, antigen release and presentation, activation of T-cell responses, lymphocytic infiltration into tumors and depletion of immunosuppression. Potential synergistic combinations include checkpoint blockade with conventional (radiation, chemotherapy and targeted therapies) and newer immunotherapies (cancer vaccines, oncolytic viruses, among others). Reliable biomarkers are necessary to define patients who will achieve best clinical benefit with minimal toxicity in combination therapy.
Keywords: checkpoint inhibitors; combination therapies; cytotoxic T-lymphocyte antigen 4 (CTLA-4); immunotherapy; malignancy; programmed death receptor-1 (PD-1) and ligand-1 (PD-L1).
Conflict of interest statement
MA Postow has received research support from Bristol-Myers Squibb and has served on advisory councils. MA Postow has also received honoraria from Bristol-Myers Squibb and Merck. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Figures
Similar articles
-
Immune checkpoint modulation: rational design of combination strategies.Pharmacol Ther. 2015 Jun;150:23-32. doi: 10.1016/j.pharmthera.2015.01.003. Epub 2015 Jan 10. Pharmacol Ther. 2015. PMID: 25583297 Review.
-
Checkpoint blockade for cancer therapy: revitalizing a suppressed immune system.Trends Mol Med. 2015 Aug;21(8):482-91. doi: 10.1016/j.molmed.2015.05.005. Epub 2015 Jun 16. Trends Mol Med. 2015. PMID: 26091825 Review.
-
The Evolving Role of Immune Checkpoint Inhibitors in Cancer Treatment.Oncologist. 2015 Jul;20(7):812-22. doi: 10.1634/theoncologist.2014-0422. Epub 2015 Jun 11. Oncologist. 2015. PMID: 26069281 Free PMC article. Review.
-
Combination of checkpoint inhibitors with other agents as a strategy to improve anti-cancer effect - a glimpse to the future.Expert Opin Investig Drugs. 2018 Jul;27(7):569-572. doi: 10.1080/13543784.2018.1494724. Epub 2018 Jul 6. Expert Opin Investig Drugs. 2018. PMID: 29958097
-
Targeted Therapy and Checkpoint Immunotherapy Combinations for the Treatment of Cancer.Trends Immunol. 2016 Jul;37(7):462-476. doi: 10.1016/j.it.2016.04.010. Epub 2016 May 20. Trends Immunol. 2016. PMID: 27216414 Review.
Cited by
-
Association of Survival and Immune-Related Adverse Events With Anti-PD-1/PD-L1 and Anti-CTLA-4 Inhibitors, Alone or Their Combination for the Treatment of Cancer: A Systematic Review and Meta-Analysis of 13 Clinical Trials.Front Oncol. 2021 Feb 25;11:575457. doi: 10.3389/fonc.2021.575457. eCollection 2021. Front Oncol. 2021. PMID: 33718135 Free PMC article.
-
Cancer immunotherapy using a polysaccharide from Codium fragile in a murine model.Oncoimmunology. 2020 Jun 1;9(1):1772663. doi: 10.1080/2162402X.2020.1772663. Oncoimmunology. 2020. PMID: 32923129 Free PMC article.
-
From CheckMate 227 to CheckMate 9LA: rethinking the status of chemotherapy in the immunotherapy era-chemo-free or chemo-reform?Transl Lung Cancer Res. 2021 Apr;10(4):1924-1927. doi: 10.21037/tlcr-21-179. Transl Lung Cancer Res. 2021. PMID: 34012802 Free PMC article. No abstract available.
-
Fusogenic Viruses in Oncolytic Immunotherapy.Cancers (Basel). 2018 Jun 26;10(7):216. doi: 10.3390/cancers10070216. Cancers (Basel). 2018. PMID: 29949934 Free PMC article. Review.
-
Cholesterol Metabolism as a Potential Therapeutic Target and a Prognostic Biomarker for Cancer Immunotherapy.Onco Targets Ther. 2021 Jun 21;14:3803-3812. doi: 10.2147/OTT.S315998. eCollection 2021. Onco Targets Ther. 2021. PMID: 34188488 Free PMC article. Review.
References
-
- Seiwert TY, Burtness B, Weiss J, et al. A Phase 1 b study of MK-3475 in patients with human papillomavirus (HPV)-associated and non-HPV associated head and neck (H/N) cancer. J. Clin. Oncol. 2014;32(5s) Abstract 6011.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials