

The Epidemiology of Hand, Foot and Mouth Disease in Asia: A Systematic Review and Analysis
- PMID: 27273688
- PMCID: PMC5130063
- DOI: 10.1097/INF.0000000000001242
The Epidemiology of Hand, Foot and Mouth Disease in Asia: A Systematic Review and Analysis
Abstract
Context: Hand, foot and mouth disease (HFMD) is a widespread pediatric disease caused primarily by human enterovirus 71 (EV-A71) and Coxsackievirus A16 (CV-A16).
Objective: This study reports a systematic review of the epidemiology of HFMD in Asia.
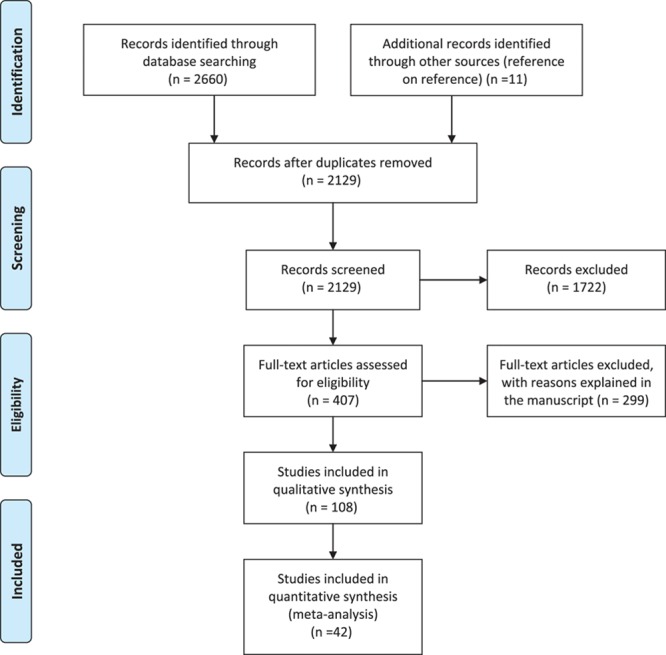
Data sources: PubMed, Web of Science and Google Scholar were searched up to December 2014.
Study selection: Two reviewers independently assessed studies for epidemiologic and serologic information about prevalence and incidence of HFMD against predetermined inclusion/exclusion criteria.
Data extraction: Two reviewers extracted answers for 8 specific research questions on HFMD epidemiology. The results are checked by 3 others.
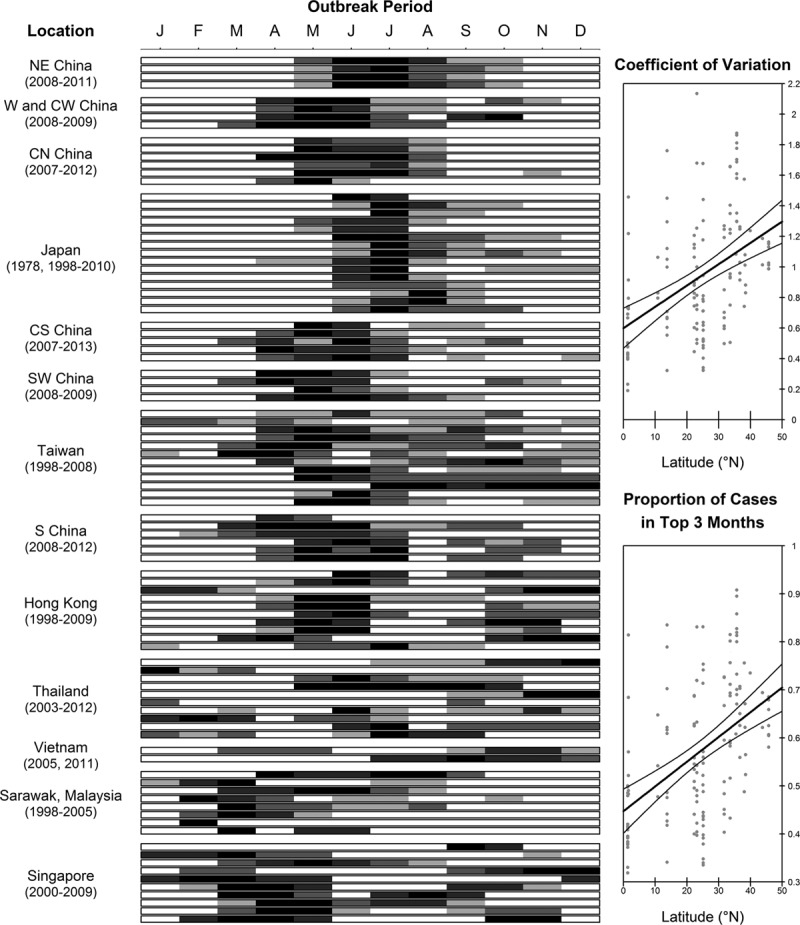
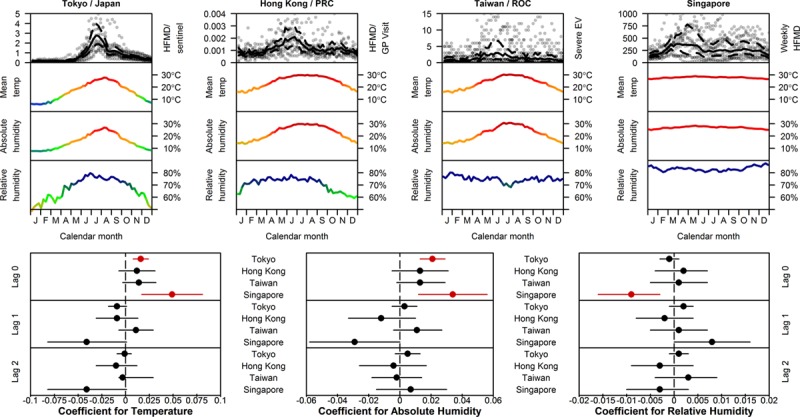
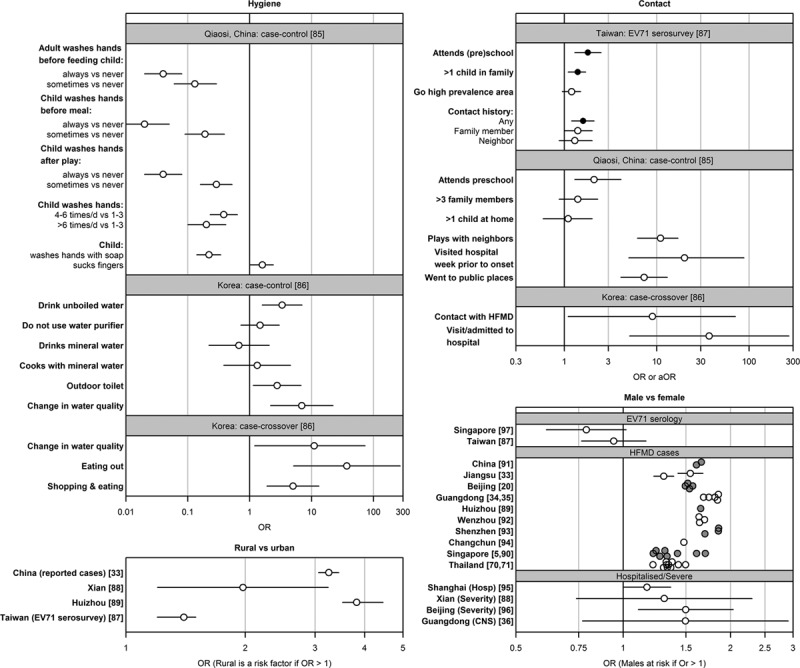
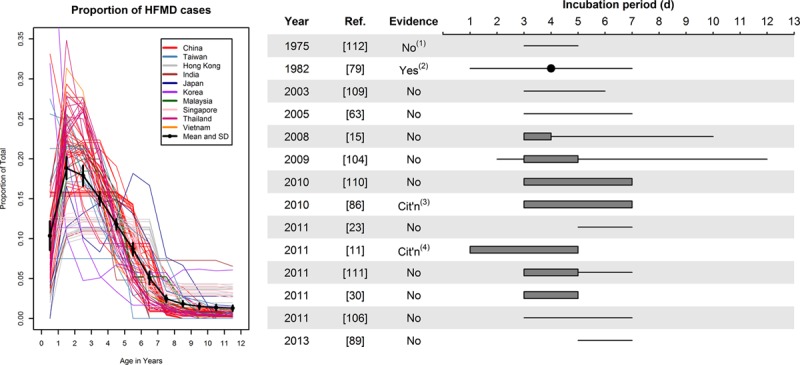
Results: HFMD is found to be seasonal in temperate Asia with a summer peak and in subtropical Asia with spring and fall peaks, but not in tropical Asia; evidence of a climatic role was identified for temperate Japan. Risk factors for HFMD include hygiene, age, gender and social contacts, but most studies were underpowered to adjust rigorously for confounding variables. Both community-level and school-level transmission have been implicated, but their relative importance for HFMD is inconclusive. Epidemiologic indices are poorly understood: No supporting quantitative evidence was found for the incubation period of EV-A71; the symptomatic rate of EV-A71/Coxsackievirus A16 infection was from 10% to 71% in 4 studies; while the basic reproduction number was between 1.1 and 5.5 in 3 studies. The uncertainty in these estimates inhibits their use for further analysis.
Limitations: Diversity of study designs complicates attempts to identify features of HFMD epidemiology.
Conclusions: Knowledge on HFMD remains insufficient to guide interventions such as the incorporation of an EV-A71 vaccine in pediatric vaccination schedules. Research is urgently needed to fill these gaps.
Conflict of interest statement
Supported by Singapore’s Ministry of Health Services Research (HSRG12MAY023), Communicable Disease Public Health Research (CDPHRG12NOV021), the Centre for Infectious Disease Epidemiology and Research, the Ministry of Education Tier 1 grant and the President’s Graduate Fellowship to W.M.K. The funders had no role in the decision to publish. T.B. is employed by commercial company, Standard Analytics. The remaining authors have no financial relationships relevant to this article to disclose. The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Hand, Foot, and Mouth Disease in China: Modeling Epidemic Dynamics of Enterovirus Serotypes and Implications for Vaccination.PLoS Med. 2016 Feb 16;13(2):e1001958. doi: 10.1371/journal.pmed.1001958. eCollection 2016 Feb. PLoS Med. 2016. PMID: 26882540 Free PMC article.
-
Molecular epidemiology and clinical features of hand, foot and mouth disease in northern Thailand in 2016: a prospective cohort study.BMC Infect Dis. 2018 Dec 6;18(1):630. doi: 10.1186/s12879-018-3560-4. BMC Infect Dis. 2018. PMID: 30522440 Free PMC article.
-
Basic Reproduction Number of Enterovirus 71 and Coxsackievirus A16 and A6: Evidence From Outbreaks of Hand, Foot, and Mouth Disease in China Between 2011 and 2018.Clin Infect Dis. 2021 Nov 2;73(9):e2552-e2559. doi: 10.1093/cid/ciaa1853. Clin Infect Dis. 2021. PMID: 33320199
-
The History of Enterovirus A71 Outbreaks and Molecular Epidemiology in the Asia-Pacific Region.J Biomed Sci. 2019 Oct 18;26(1):75. doi: 10.1186/s12929-019-0573-2. J Biomed Sci. 2019. PMID: 31627753 Free PMC article. Review.
-
[Prevalence and Analyses of the Changing Etiology of Hand, Foot and Mouth Disease in China].Bing Du Xue Bao. 2015 Sep;31(5):554-9. Bing Du Xue Bao. 2015. PMID: 26738295 Review. Chinese.
Cited by
-
Spatial and Temporal Characteristics of Hand-Foot-and-Mouth Disease and Its Response to Climate Factors in the Ili River Valley Region of China.Int J Environ Res Public Health. 2021 Feb 17;18(4):1954. doi: 10.3390/ijerph18041954. Int J Environ Res Public Health. 2021. PMID: 33671423 Free PMC article.
-
A hSCARB2-transgenic mouse model for Coxsackievirus A16 pathogenesis.Virol J. 2021 Apr 21;18(1):84. doi: 10.1186/s12985-021-01557-5. Virol J. 2021. PMID: 33882964 Free PMC article.
-
Temporal relationships between climate variables and hand-foot-mouth disease: a multi-province study in the Mekong Delta Region, Vietnam.Int J Biometeorol. 2020 Mar;64(3):389-396. doi: 10.1007/s00484-019-01824-9. Epub 2019 Nov 12. Int J Biometeorol. 2020. PMID: 31720856
-
Spatial-temporal-demographic and virological changes of hand, foot and mouth disease incidence after vaccination in a vulnerable region of China.BMC Public Health. 2022 Aug 1;22(1):1468. doi: 10.1186/s12889-022-13860-z. BMC Public Health. 2022. PMID: 35915424 Free PMC article.
-
Molecular epidemiology of coxsackievirus A16 circulating in children in Beijing, China from 2010 to 2019.World J Pediatr. 2021 Oct;17(5):508-516. doi: 10.1007/s12519-021-00451-y. Epub 2021 Aug 28. World J Pediatr. 2021. PMID: 34453285 Free PMC article.
References
-
- Huang MC, Wang SM, Hsu YW, et al. Long-term cognitive and motor deficits after enterovirus 71 brainstem encephalitis in children. Pediatrics. 2006;118:e1785–e1788. - PubMed
-
- Chang LY, Huang LM, Gau SS, et al. Neurodevelopment and cognition in children after enterovirus 71 infection. N Engl J Med. 2007;356:1226–1234. - PubMed
-
- World Health Organization Western Pacific Region. Hand, foot, and mouth disease situation update. 2014. Dec 29, Available at: http://www.wpro.who.int/emerging_diseases/hfmd_biweekly_29dec2014.pdf?ua=1. Accessed March 11, 2015.
-
- Ang LW, Koh BK, Chan KP, et al. Epidemiology and control of hand, foot and mouth disease in Singapore, 2001–2007. Ann Acad Med Singapore. 2009;38:106–112. - PubMed
-
- Chen SP, Huang YC, Li WC, et al. Comparison of clinical features between coxsackievirus A2 and enterovirus 71 during the enterovirus outbreak in Taiwan, 2008: a children’s hospital experience. J Microbiol Immunol Infect. 2010;43:99–104. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
