

Increased GVHD-related mortality with broad-spectrum antibiotic use after allogeneic hematopoietic stem cell transplantation in human patients and mice
- PMID: 27194729
- PMCID: PMC4991773
- DOI: 10.1126/scitranslmed.aaf2311
Increased GVHD-related mortality with broad-spectrum antibiotic use after allogeneic hematopoietic stem cell transplantation in human patients and mice
Abstract
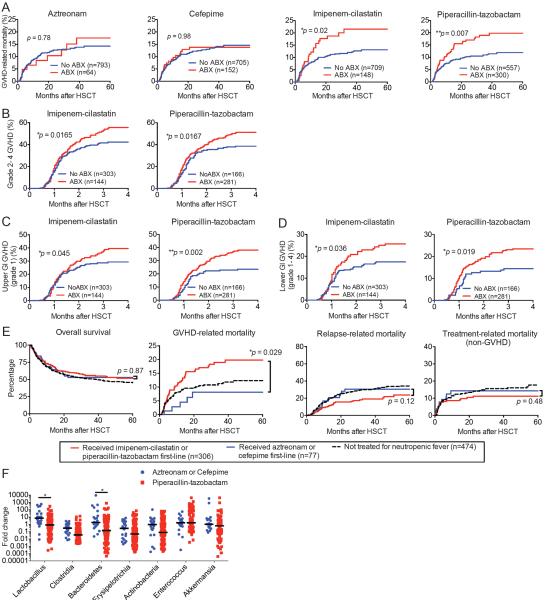
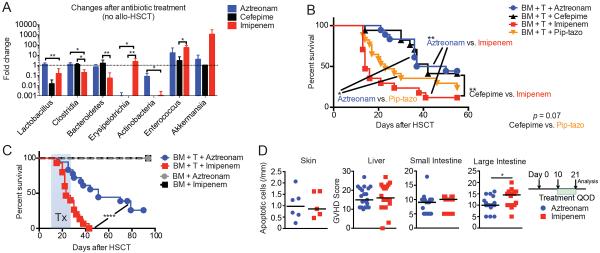
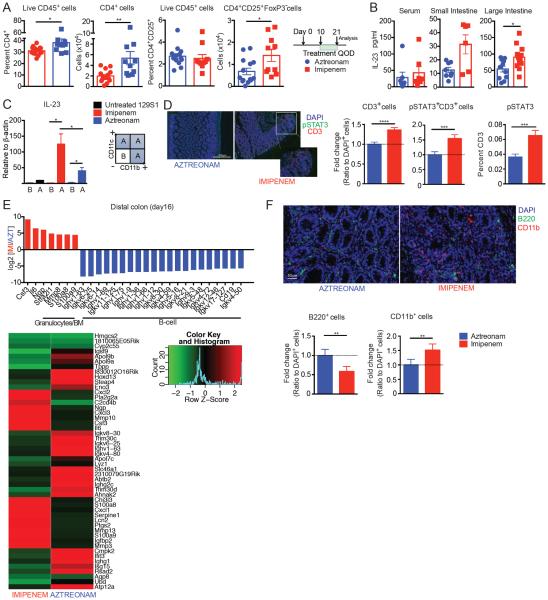
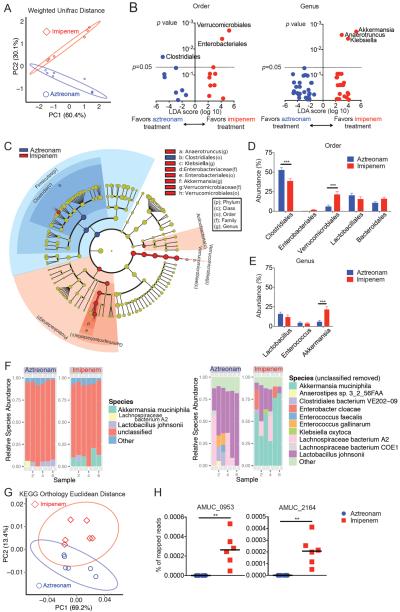
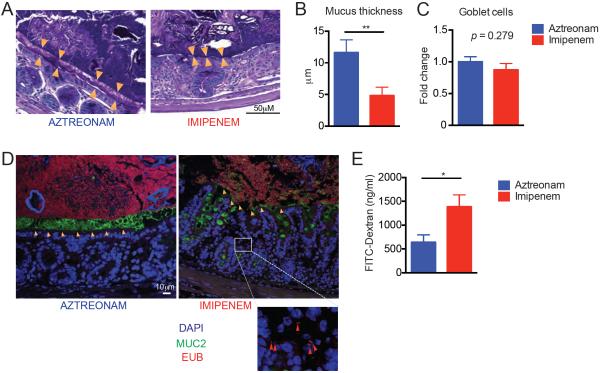
Intestinal bacteria may modulate the risk of infection and graft-versus-host disease (GVHD) after allogeneic hematopoietic stem cell transplantation (allo-HSCT). Allo-HSCT recipients often develop neutropenic fever, which is treated with antibiotics that may target anaerobic bacteria in the gut. We retrospectively examined 857 allo-HSCT recipients and found that treatment of neutropenic fever with imipenem-cilastatin and piperacillin-tazobactam antibiotics was associated with increased GVHD-related mortality at 5 years (21.5% for imipenem-cilastatin-treated patients versus 13.1% for untreated patients, P = 0.025; 19.8% for piperacillin-tazobactam-treated patients versus 11.9% for untreated patients, P = 0.007). However, two other antibiotics also used to treat neutropenic fever, aztreonam and cefepime, were not associated with GVHD-related mortality (P = 0.78 and P = 0.98, respectively). Analysis of stool specimens from allo-HSCT recipients showed that piperacillin-tazobactam administration was associated with perturbation of gut microbial composition. Studies in mice demonstrated aggravated GVHD mortality with imipenem-cilastatin or piperacillin-tazobactam compared to aztreonam (P < 0.01 and P < 0.05, respectively). We found pathological evidence for increased GVHD in the colon of imipenem-cilastatin-treated mice (P < 0.05), but no difference in the concentration of short-chain fatty acids or numbers of regulatory T cells. Notably, imipenem-cilastatin treatment of mice with GVHD led to loss of the protective mucus lining of the colon (P < 0.01) and the compromising of intestinal barrier function (P < 0.05). Sequencing of mouse stool specimens showed an increase in Akkermansia muciniphila (P < 0.001), a commensal bacterium with mucus-degrading capabilities, raising the possibility that mucus degradation may contribute to murine GVHD. We demonstrate an underappreciated risk for the treatment of allo-HSCT recipients with antibiotics that may exacerbate GVHD in the colon.
Copyright © 2016, American Association for the Advancement of Science.
Figures
Similar articles
-
[Gut microbiota and graft-versus-host disease: broad-spectrum antibiotic use increases post-allogeneic hematopoietic stem cell transplant graft-versus-host disease-related mortality].Rinsho Ketsueki. 2017;58(7):835-842. doi: 10.11406/rinketsu.58.835. Rinsho Ketsueki. 2017. PMID: 28781282 Japanese.
-
Piperacillin-tazobactam vs. imipenem-cilastatin as empirical therapy in hematopoietic stem cell transplantation recipients with febrile neutropenia.Clin Transplant. 2016 Mar;30(3):263-9. doi: 10.1111/ctr.12685. Epub 2016 Feb 2. Clin Transplant. 2016. PMID: 26701371 Clinical Trial.
-
Imipenem/cilastatin versus piperacillin/tazobactam plus amikacin for empirical therapy in febrile neutropenic patients: results of the COSTINE study.Curr Med Res Opin. 2005 May;21(5):645-55. doi: 10.1185/030079905X43631. Curr Med Res Opin. 2005. PMID: 15969864 Clinical Trial.
-
Gut microbiota injury in allogeneic haematopoietic stem cell transplantation.Nat Rev Cancer. 2018 May;18(5):283-295. doi: 10.1038/nrc.2018.10. Epub 2018 Feb 16. Nat Rev Cancer. 2018. PMID: 29449660 Free PMC article. Review.
-
The treatment of severe intra-abdominal infections: the role of piperacillin/tazobactam.Intensive Care Med. 1994 Jul;20 Suppl 3:S35-8. doi: 10.1007/BF01745249. Intensive Care Med. 1994. PMID: 7962987 Review.
Cited by
-
Reg3α concentrations at day of allogeneic stem cell transplantation predict outcome and correlate with early antibiotic use.Blood Adv. 2023 Apr 11;7(7):1326-1335. doi: 10.1182/bloodadvances.2022008480. Blood Adv. 2023. PMID: 36350750 Free PMC article.
-
Allogeneic hematopoietic cell transplantation, the microbiome, and graft-versus-host disease.Gut Microbes. 2023 Jan-Dec;15(1):2178805. doi: 10.1080/19490976.2023.2178805. Gut Microbes. 2023. PMID: 36794370 Free PMC article. Review.
-
Emerging roles of the gut microbiota in cancer immunotherapy.Front Immunol. 2023 Feb 22;14:1139821. doi: 10.3389/fimmu.2023.1139821. eCollection 2023. Front Immunol. 2023. PMID: 36911704 Free PMC article. Review.
-
Reconstitution of the gut microbiota of antibiotic-treated patients by autologous fecal microbiota transplant.Sci Transl Med. 2018 Sep 26;10(460):eaap9489. doi: 10.1126/scitranslmed.aap9489. Sci Transl Med. 2018. PMID: 30257956 Free PMC article. Clinical Trial.
-
Bacterial blood stream infections (BSIs), particularly post-engraftment BSIs, are associated with increased mortality after allogeneic hematopoietic cell transplantation.Bone Marrow Transplant. 2019 Aug;54(8):1254-1265. doi: 10.1038/s41409-018-0401-4. Epub 2018 Dec 13. Bone Marrow Transplant. 2019. PMID: 30546070 Free PMC article.
References
-
- Meyers JD. Infection in bone marrow transplant recipients. The American journal of medicine. 1986;81:27–38. - PubMed
-
- Wingard JR. Opportunistic infections after blood and marrow transplantation. Transplant infectious disease : an official journal of the Transplantation Society. 1999;1:3–20. - PubMed
-
- Hiemenz JW. Management of infections complicating allogeneic hematopoietic stem cell transplantation. Seminars in hematology. 2009;46:289–312. - PubMed
-
- Freifeld AG, Bow EJ, Sepkowitz KA, Boeckh MJ, Ito JI, Mullen CA, Raad II, Rolston KV, Young JA, Wingard JR. A. Infectious Diseases Society of, Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2011;52:e56–93. - PubMed
MeSH terms
Substances
Grants and funding
- R01 AI101406/AI/NIAID NIH HHS/United States
- R01 HL069929/HL/NHLBI NIH HHS/United States
- R01 HL124112/HL/NHLBI NIH HHS/United States
- R01 AI080455/AI/NIAID NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- R00 CA176376/CA/NCI NIH HHS/United States
- R01 HL125571/HL/NHLBI NIH HHS/United States
- R01 AI100288/AI/NIAID NIH HHS/United States
- K08 HL115355/HL/NHLBI NIH HHS/United States
- R01 HL123340/HL/NHLBI NIH HHS/United States
- P01 CA023766/CA/NCI NIH HHS/United States
- K08 CA184420/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
