

Review
doi: 10.1038/nri.2016.19.
Epub 2016 Mar 14.
Paediatric HIV infection: the potential for cure
Affiliations
- PMID: 26972723
- PMCID: PMC5694689
- DOI: 10.1038/nri.2016.19
Item in Clipboard
Review
Paediatric HIV infection: the potential for cure
Nat Rev Immunol.
2016 Apr.
Abstract
Recent anecdotal reports of HIV-infected children who received early antiretroviral therapy (ART) and showed sustained control of viral replication even after ART discontinuation have raised the question of whether there is greater intrinsic potential for HIV remission, or even eradication ('cure'), in paediatric infection than in adult infection. This Review describes the influence of early initiation of ART, of immune ontogeny and of maternal factors on the potential for HIV cure in children and discusses the unique immunotherapeutic opportunities and obstacles that paediatric infection may present.
Conflict of interest statement
The authors declare no competing interests.
Figures
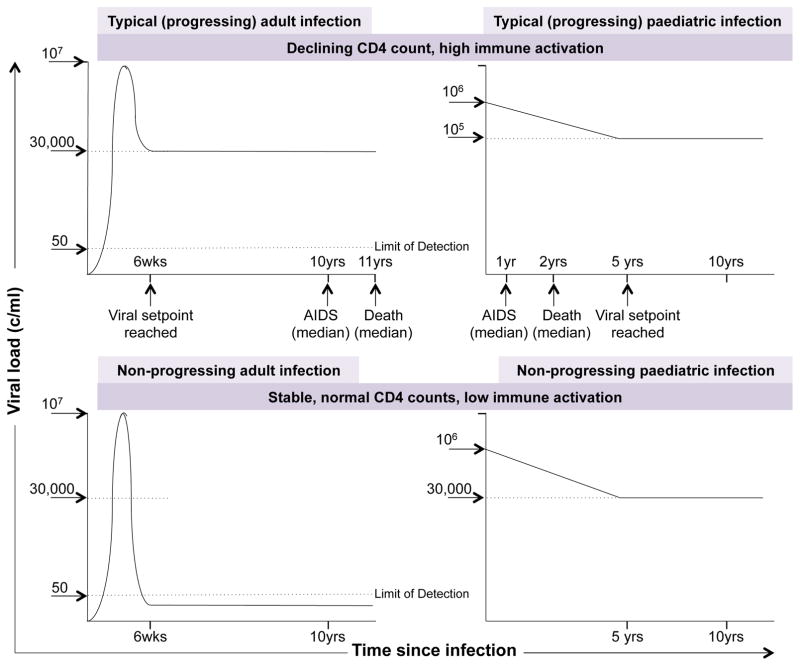
Typical, progressing adult and paediatric infection (upper panels), and non-progressing adult and paediatric infection (lower panels),,,. Typically, in HIV infection of ART-naïve adults, a viral setpoint is reached after 6 weeks and the median time to AIDS is 10 years. In typical, ART-naïve paediatric HIV infection, a viral setpoint is reached after 5 years and the median time to AIDS is 1 year. Non-progressing adult infection is characterised by low/undetectable viral loads and low levels of immune activation. The prevalence of non-progressing paediatric infection is 5–10% [ref 7,158,159], and of adult elite control ~0.3% [ref 146]. Non-progressing paediatric infection also features low levels of immune activation, but in the setting of high viral loads (~30,000 copies/ml).
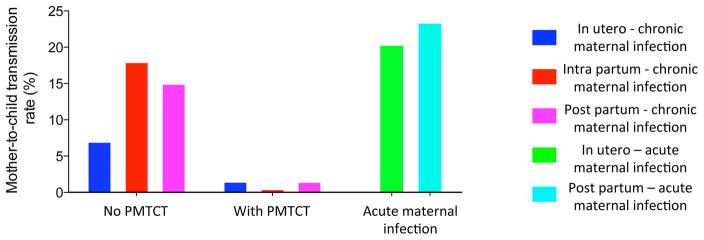
Mother-to-child transmission (MTCT) risk of HIV in the absence of prophylactic measures is approximately 7% from in utero infection, 18% from intra-partum infection, and 15% from post-partum transmission (through breast-milk; breast-feeding for 18–24 months)–. In utero-infected infants are viraemic and HIV DNA positive at birth, whereas transmission arising at the time of delivery (intra-partum) results in viraemia only some 4 weeks later. Treatment with ART of all mothers testing HIV-positive in pregnancy has reduced combined in utero and intra-partum MTCT from 25% to 1–2% [ref 102], and prevention of breast-milk transmission via ART also has reduced post-partum MTCT rates to 1–2% [ref 164]. The remaining 1–2% MTCT rate results either from ART non-adherence or from acute infection during pregnancy or after birth (in utero MTCT risk of ~20% [refs 163,165,166] or post-partum MTCT risk of 20–25% [ref 167]), since tests to detect HIV antibody are negative during acute maternal infection when peak viraemia is ~107 copies/ml and transmission risk is high.
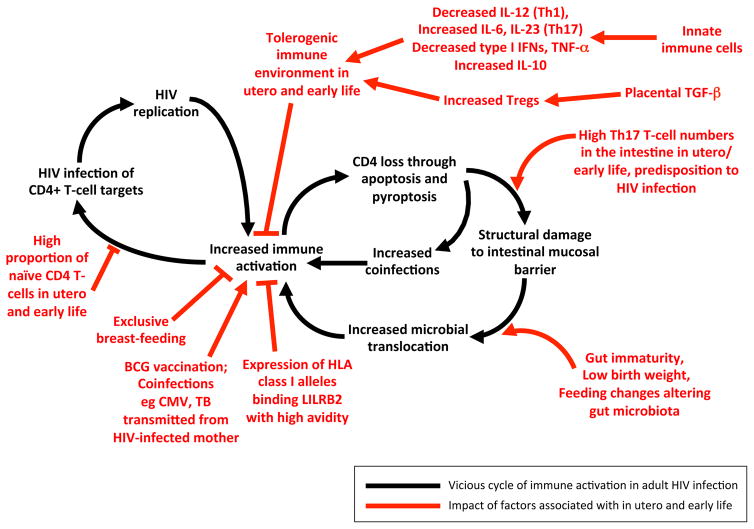
The vicious cycle of HIV infection — resulting in intestinal mucosal damage, microbial translocation across the intestinal barrier and increased immune activation, leading to increased CD4+ T-cell decline, which predisposes to further co-infections, increased immune activation, HIV replication and CD4+ T cell loss — can be prevented by the initiation of antiretroviral therapy sufficiently early in adult and paediatric infection. There are factors specific to paediatric infection that tend to interfere with this vicious cycle, and others that contribute to it, the balance of which may vary between individuals and also may depend crucially on the timing of ART initiation. Aspects of immune ontogeny that favour decreased immune activation include the tolerogenic immune environment in utero and in early life and the high proportion of naïve CD4+ T-cells. Aspects of immune ontogeny that tend to decrease paediatric cure potential include the large number of TH17 cells in the intestinal mucosa. Maternal factors favouring paediatric cure potential include maternal health, exclusive breast-feeding, lack of co-infections, and expression of HLA class I molecules that bind LILRB2 with high avidity.
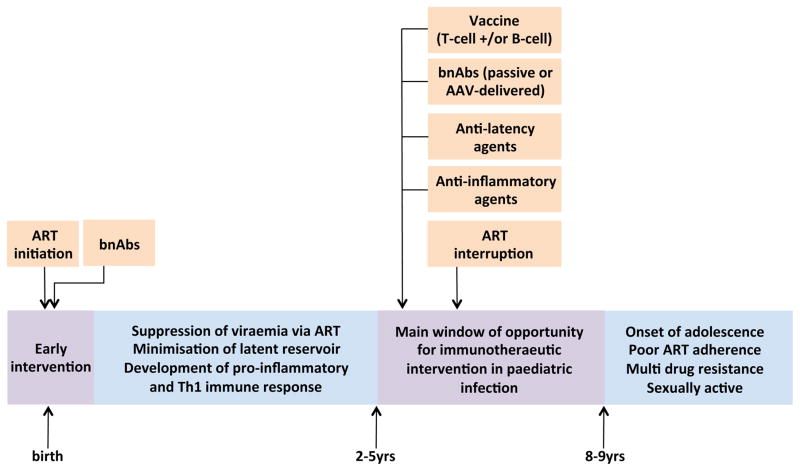
In utero paediatric infection provides particular opportunities for ART to be initiated with or without additional interventions (such as broadly neutralising antibodies) very early in the course of infection. As cell-mediated immunity is likely to have a key role in eradication of the viral reservoir, and TH1 cell responses take some years to develop fully, a period of time on ART alone may be useful to minimise the size of the viral reservoir prior to further interventions designed to eradicate infection. In late childhood, approximately between the ages of 3 and 9 yrs, immune ontogeny favours the generation of effective CD8+ T-cell immunity, which provides a window of opportunity for therapeutic intervention before the onset of puberty with associated behavioural changes including loss of ART adherence and onset of sexual activity.
Similar articles
-
Anti-retroviral therapy failure in HIV-1 infected pregnant women and its associated risk of HIV transmission.Arch Gynecol Obstet. 2020 Nov;302(5):1229-1235. doi: 10.1007/s00404-020-05743-8. Epub 2020 Aug 14. Arch Gynecol Obstet. 2020. PMID: 32803392
-
Evidence for extended age dependent maternal immunity in infected children: mother to child transmission of HIV infection and potential interventions including sulfatides of the human fetal adnexa and complementary or alternative medicines.J Stem Cells. 2012;7(3):127-53. J Stem Cells. 2012. PMID: 23619381
-
Antiretroviral therapy (ART) for treating HIV infection in ART-eligible pregnant women.Cochrane Database Syst Rev. 2010 Mar 17;(3):CD008440. doi: 10.1002/14651858.CD008440. Cochrane Database Syst Rev. 2010. PMID: 20238370 Review.
-
Maternal and infant factors and lymphocyte, CD4 and CD8 cell counts in uninfected children of HIV-1-infected mothers.AIDS. 2005 Jul 1;19(10):1071-9. doi: 10.1097/01.aids.0000174454.63250.22. AIDS. 2005. PMID: 15958839
-
Prevention of perinatal HIV transmission during pregnancy.J Antimicrob Chemother. 2000 Nov;46(5):657-68. doi: 10.1093/jac/46.5.657. J Antimicrob Chemother. 2000. PMID: 11062184 Review.
Cited by
-
12-month outcomes of HIV-infected infants identified at birth at one maternity site in Johannesburg, South Africa: an observational cohort study.Lancet HIV. 2018 Dec;5(12):e706-e714. doi: 10.1016/S2352-3018(18)30251-0. Epub 2018 Nov 8. Lancet HIV. 2018. PMID: 30416043 Free PMC article.
-
Differential Pathogen-Specific Immune Reconstitution in Antiretroviral Therapy-Treated Human Immunodeficiency Virus-Infected Children.J Infect Dis. 2019 Apr 16;219(9):1407-1417. doi: 10.1093/infdis/jiy668. J Infect Dis. 2019. PMID: 30624717 Free PMC article.
-
Viral Characteristics Associated with Maintenance of Elite Neutralizing Activity in Chronically HIV-1 Clade C-Infected Monozygotic Pediatric Twins.J Virol. 2019 Aug 13;93(17):e00654-19. doi: 10.1128/JVI.00654-19. Print 2019 Sep 1. J Virol. 2019. PMID: 31217240 Free PMC article.
-
Early treatment regimens achieve sustained virologic remission in infant macaques infected with SIV at birth.Nat Commun. 2022 Aug 16;13(1):4823. doi: 10.1038/s41467-022-32554-z. Nat Commun. 2022. PMID: 35973985 Free PMC article.
-
Recovery of effective HIV-specific CD4+ T-cell activity following antiretroviral therapy in paediatric infection requires sustained suppression of viraemia.AIDS. 2018 Jul 17;32(11):1413-1422. doi: 10.1097/QAD.0000000000001844. AIDS. 2018. PMID: 29734220 Free PMC article.
References
-
- Newell ML, et al. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet. 2004;364:1236–1243. - PubMed
-
- Collaborative Group on AIDS Incubation and HIV Survival including the CASCADE EU Concerted Action. Concerted Action on SeroConversion to AIDS and Death in Europe. Time from HIV-1 seroconversion to AIDS and death before widespread use of highly-active antiretroviral therapy: a collaborative re-analysis. Lancet. 2000;355:1131–1137. - PubMed
-
- Kaslow RA, et al. Influence of combinations of human major histocompatibility complex genes on the course of HIV-1 infection. Nature Med. 1996;2:405–411. - PubMed
-
- Kiepiela P, et al. CD8+ T-cell responses to different HIV proteins have discordant associations with viral load. Nature Med. 2007;13:46–53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
