

Alkaline Phosphatase and Hypophosphatasia
- PMID: 26590809
- PMCID: PMC4824800
- DOI: 10.1007/s00223-015-0079-1
Alkaline Phosphatase and Hypophosphatasia
Abstract
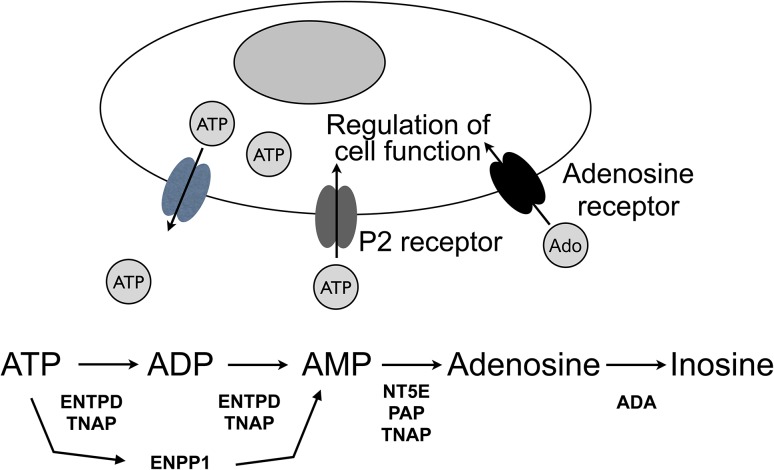
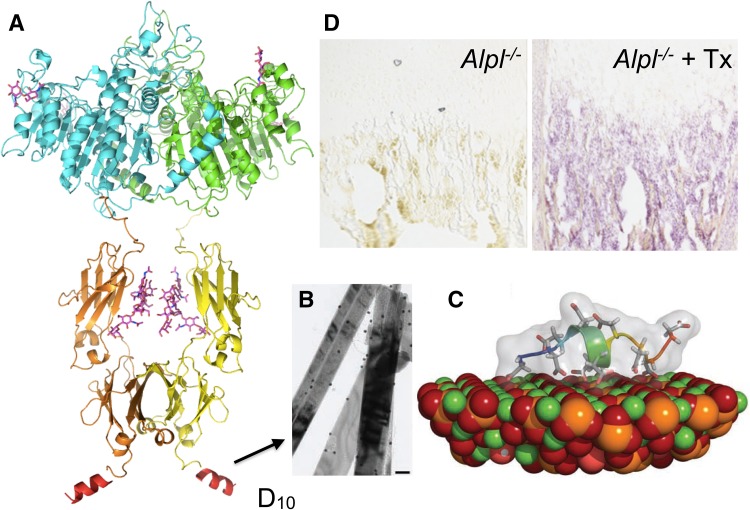
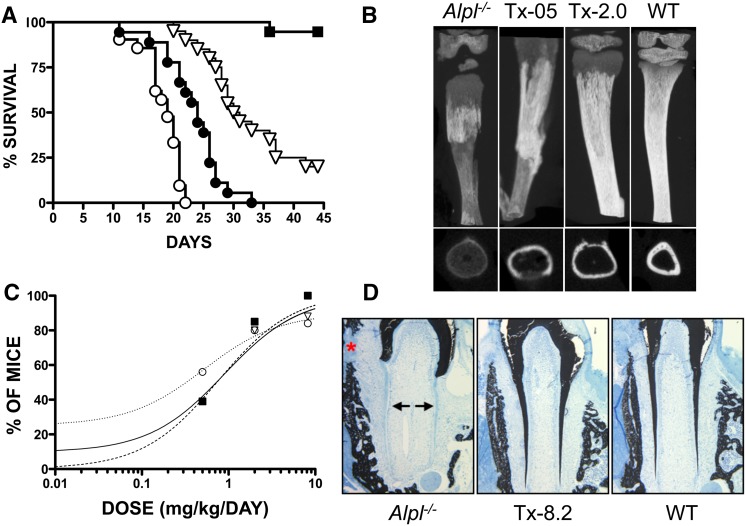
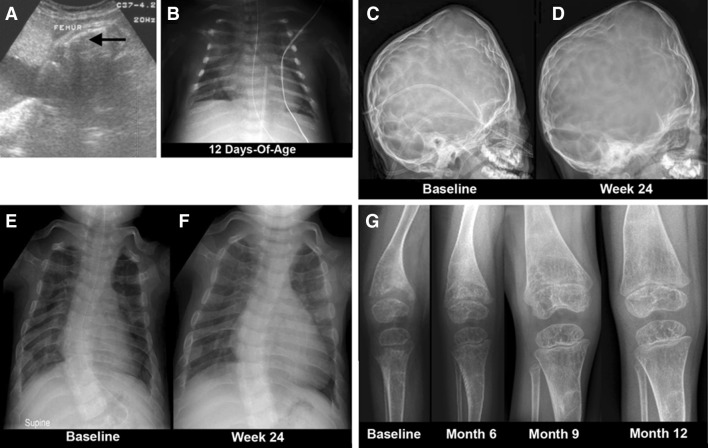
Hypophosphatasia (HPP) results from ALPL mutations leading to deficient activity of the tissue-non-specific alkaline phosphatase isozyme (TNAP) and thereby extracellular accumulation of inorganic pyrophosphate (PPi), a natural substrate of TNAP and potent inhibitor of mineralization. Thus, HPP features rickets or osteomalacia and hypomineralization of teeth. Enzyme replacement using mineral-targeted TNAP from birth prevented severe HPP in TNAP-knockout mice and was then shown to rescue and substantially treat infants and young children with life-threatening HPP. Clinical trials are revealing aspects of HPP pathophysiology not yet fully understood, such as craniosynostosis and muscle weakness when HPP is severe. New treatment approaches are under development to improve patient care.
Keywords: Calcification; Enzyme replacement; Osteomalacia; Rickets; Seizures.
Figures
Similar articles
-
Improvement of the skeletal and dental hypophosphatasia phenotype in Alpl-/- mice by administration of soluble (non-targeted) chimeric alkaline phosphatase.Bone. 2015 Mar;72:137-47. doi: 10.1016/j.bone.2014.11.017. Epub 2014 Nov 26. Bone. 2015. PMID: 25433339 Free PMC article.
-
Gene Therapy Using Adeno-Associated Virus Serotype 8 Encoding TNAP-D10 Improves the Skeletal and Dentoalveolar Phenotypes in Alpl-/- Mice.J Bone Miner Res. 2021 Sep;36(9):1835-1849. doi: 10.1002/jbmr.4382. Epub 2021 Jun 15. J Bone Miner Res. 2021. PMID: 34076297 Free PMC article.
-
Multisystemic functions of alkaline phosphatases.Methods Mol Biol. 2013;1053:27-51. doi: 10.1007/978-1-62703-562-0_3. Methods Mol Biol. 2013. PMID: 23860646 Review.
-
Enzyme replacement prevents enamel defects in hypophosphatasia mice.J Bone Miner Res. 2012 Aug;27(8):1722-34. doi: 10.1002/jbmr.1619. J Bone Miner Res. 2012. PMID: 22461224 Free PMC article.
-
Tissue-Nonspecific Alkaline Phosphatase-A Gatekeeper of Physiological Conditions in Health and a Modulator of Biological Environments in Disease.Biomolecules. 2020 Dec 8;10(12):1648. doi: 10.3390/biom10121648. Biomolecules. 2020. PMID: 33302551 Free PMC article. Review.
Cited by
-
A novel de novo heterozygous ALPL nonsense mutation associated with adult hypophosphatasia.Osteoporos Int. 2020 Nov;31(11):2251-2257. doi: 10.1007/s00198-020-05490-1. Epub 2020 Jun 23. Osteoporos Int. 2020. PMID: 32572521 Free PMC article.
-
The Elusive Origin of Atherosclerotic Plaque Calcification.Front Cell Dev Biol. 2021 Mar 9;9:622736. doi: 10.3389/fcell.2021.622736. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 33768090 Free PMC article. Review.
-
Determination of serum alkaline phosphatase reference in healthy children aged 1-18 years.Caspian J Intern Med. 2022 Fall;13(4):749-756. doi: 10.22088/cjim.13.4.749. Caspian J Intern Med. 2022. PMID: 36420337 Free PMC article.
-
A new perspective on intervertebral disc calcification-from bench to bedside.Bone Res. 2024 Jan 22;12(1):3. doi: 10.1038/s41413-023-00307-3. Bone Res. 2024. PMID: 38253615 Free PMC article. Review.
-
Between a rock and a hard place: Regulation of mineralization in the periodontium.Genesis. 2022 Sep;60(8-9):e23474. doi: 10.1002/dvg.23474. Epub 2022 Apr 23. Genesis. 2022. PMID: 35460154 Free PMC article. Review.
References
-
- Robison R (1932) The significance of phosphoric esters in metabolism. New York University Press, New York
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
