

Phase I Study of the Novel Investigational NEDD8-Activating Enzyme Inhibitor Pevonedistat (MLN4924) in Patients with Relapsed/Refractory Multiple Myeloma or Lymphoma
- PMID: 26561559
- PMCID: PMC5694347
- DOI: 10.1158/1078-0432.CCR-15-1237
Phase I Study of the Novel Investigational NEDD8-Activating Enzyme Inhibitor Pevonedistat (MLN4924) in Patients with Relapsed/Refractory Multiple Myeloma or Lymphoma
Abstract
Purpose: Evaluate the safety, pharmacokinetic profile, pharmacodynamic effects, and antitumor activity of the first-in-class investigational NEDD8-activating enzyme (NAE) inhibitor pevonedistat (TAK-924/MLN4924) in patients with relapsed/refractory lymphoma or multiple myeloma.
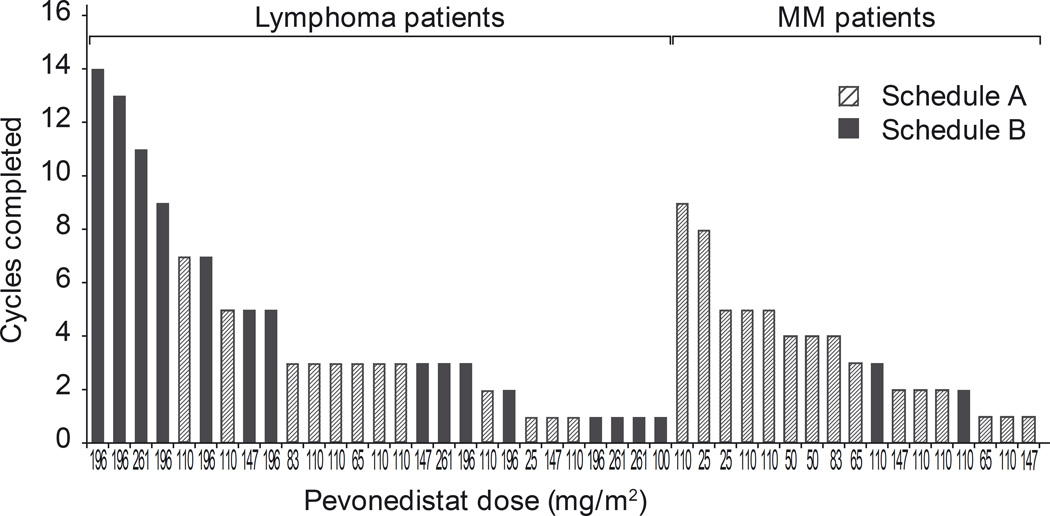
Experimental design: Patients with relapsed/refractory myeloma (n = 17) or lymphoma (n = 27) received intravenous pevonedistat 25 to 147 mg/m(2) on days 1, 2, 8, 9 (schedule A; n = 27) or 100 to 261 mg/m(2) on days 1, 4, 8, 11 (schedule B; n = 17) of 21-day cycles.
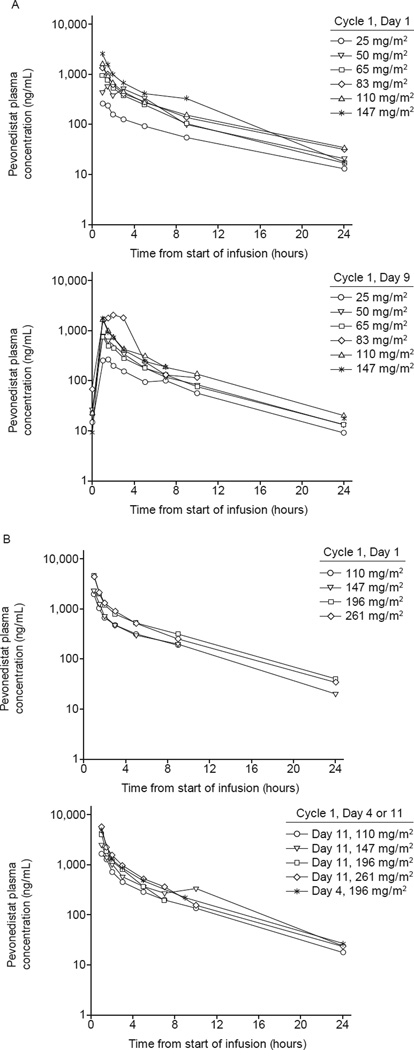
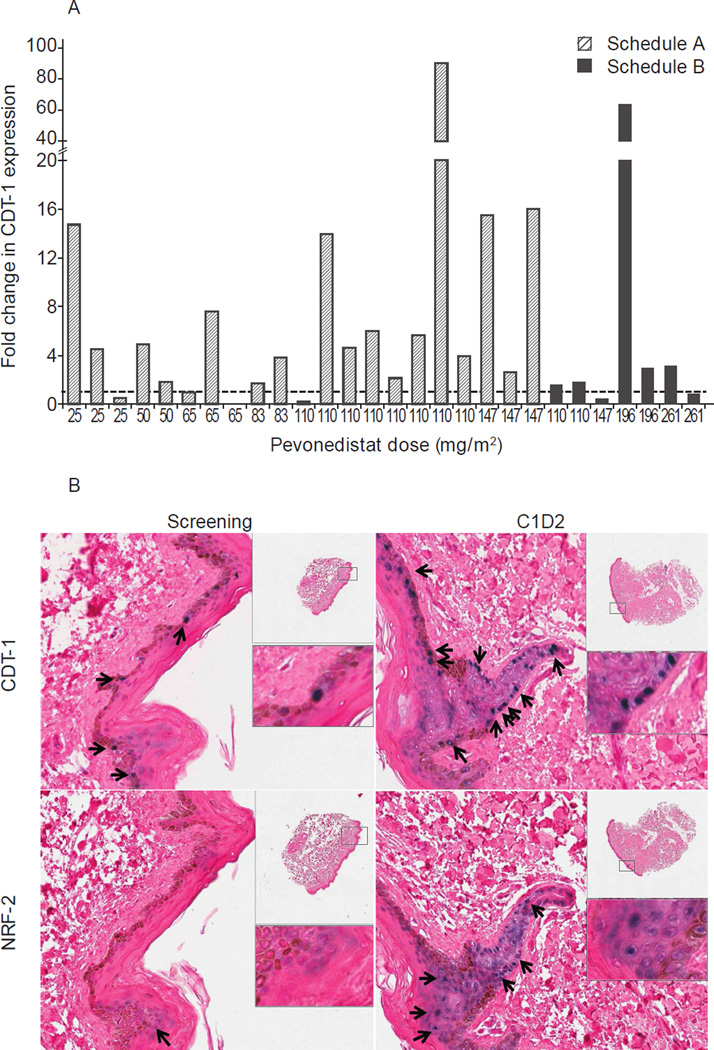
Results: Maximum tolerated doses were 110 mg/m(2) (schedule A) and 196 mg/m(2) (schedule B). Dose-limiting toxicities included febrile neutropenia, transaminase elevations, muscle cramps (schedule A), and thrombocytopenia (schedule B). Common adverse events included fatigue and nausea. Common grade ≥3 events were anemia (19%; schedule A), and neutropenia and pneumonia (12%; schedule B). Clinically significant myelosuppression was uncommon. There were no treatment-related deaths. Pevonedistat pharmacokinetics exhibited a biphasic disposition phase and approximate dose-proportional increases in systemic exposure. Consistent with the short mean elimination half-life of approximately 8.5 hours, little-to-no drug accumulation in plasma was seen after multiple dosing. Pharmacodynamic evidence of NAE inhibition included increased skin levels of CDT-1 and NRF-2 (substrates of NAE-dependent ubiquitin ligases), and increased NRF-2-regulated gene transcript levels in whole blood. Pevonedistat-NEDD8 adduct was detected in bone marrow aspirates, indicating pevonedistat target engagement in the bone marrow compartment. Three lymphoma patients had partial responses; 30 patients achieved stable disease.
Conclusions: Pevonedistat demonstrated anticipated pharmacodynamic effects in the clinical setting, a tolerable safety profile, and some preliminary evidence that may be suggestive of the potential for activity in relapsed/refractory lymphoma.
©2015 American Association for Cancer Research.
Conflict of interest statement
Figures
Similar articles
-
A phase I study of the investigational NEDD8-activating enzyme inhibitor pevonedistat (TAK-924/MLN4924) in patients with metastatic melanoma.Invest New Drugs. 2016 Aug;34(4):439-49. doi: 10.1007/s10637-016-0348-5. Epub 2016 Apr 8. Invest New Drugs. 2016. PMID: 27056178 Free PMC article. Clinical Trial.
-
Phase I Study of the Investigational NEDD8-Activating Enzyme Inhibitor Pevonedistat (TAK-924/MLN4924) in Patients with Advanced Solid Tumors.Clin Cancer Res. 2016 Feb 15;22(4):847-57. doi: 10.1158/1078-0432.CCR-15-1338. Epub 2015 Sep 30. Clin Cancer Res. 2016. PMID: 26423795 Clinical Trial.
-
Safety, tolerability, and preliminary activity of CUDC-907, a first-in-class, oral, dual inhibitor of HDAC and PI3K, in patients with relapsed or refractory lymphoma or multiple myeloma: an open-label, dose-escalation, phase 1 trial.Lancet Oncol. 2016 May;17(5):622-31. doi: 10.1016/S1470-2045(15)00584-7. Epub 2016 Mar 31. Lancet Oncol. 2016. PMID: 27049457 Free PMC article. Clinical Trial.
-
MLN4924: a novel first-in-class inhibitor of NEDD8-activating enzyme for cancer therapy.Expert Opin Investig Drugs. 2012 Oct;21(10):1563-73. doi: 10.1517/13543784.2012.707192. Epub 2012 Jul 16. Expert Opin Investig Drugs. 2012. PMID: 22799561 Review.
-
MLN4924 therapy as a novel approach in cancer treatment modalities.J Chemother. 2016 Apr;28(2):74-82. doi: 10.1179/1973947815Y.0000000066. J Chemother. 2016. PMID: 26292710 Review.
Cited by
-
The replication initiation determinant protein (RepID) modulates replication by recruiting CUL4 to chromatin.Nat Commun. 2018 Jul 17;9(1):2782. doi: 10.1038/s41467-018-05177-6. Nat Commun. 2018. PMID: 30018425 Free PMC article.
-
A patent review of the ubiquitin ligase system: 2015-2018.Expert Opin Ther Pat. 2018 Dec;28(12):919-937. doi: 10.1080/13543776.2018.1549229. Epub 2018 Nov 23. Expert Opin Ther Pat. 2018. PMID: 30449221 Free PMC article. Review.
-
Overcoming drug resistance by targeting protein homeostasis in multiple myeloma.Cancer Drug Resist. 2021;4(4):1028-1046. doi: 10.20517/cdr.2021.93. Epub 2021 Dec 2. Cancer Drug Resist. 2021. PMID: 35265794 Free PMC article.
-
SUMOylation and related post-translational modifications in natural killer cell anti-cancer responses.Front Cell Dev Biol. 2023 May 25;11:1213114. doi: 10.3389/fcell.2023.1213114. eCollection 2023. Front Cell Dev Biol. 2023. PMID: 37313439 Free PMC article. Review.
-
Recent Advances in the Applications of Small Molecules in the Treatment of Multiple Myeloma.Int J Mol Sci. 2023 Jan 31;24(3):2645. doi: 10.3390/ijms24032645. Int J Mol Sci. 2023. PMID: 36768967 Free PMC article. Review.
References
-
- Hershko A. The ubiquitin system for protein degradation and some of its roles in the control of the cell division cycle. Cell Death Differ. 2005;12:1191–1197. - PubMed
-
- Ciechanover A. Intracellular protein degradation: from a vague idea thru the lysosome and the ubiquitin-proteasome system and onto human diseases and drug targeting. Cell Death Differ. 2005;12:1178–1190. - PubMed
-
- McBride A, Ryan PY. Proteasome inhibitors in the treatment of multiple myeloma. Expert Rev Anticancer Ther. 2013;13:339–358. - PubMed
-
- O'Connor OA, Wright J, Moskowitz C, Muzzy J, Gregor-Cortelli B, Stubblefield M, et al. Phase II clinical experience with the novel proteasome inhibitor bortezomib in patients with indolent non-Hodgkin's lymphoma and mantle cell lymphoma. J Clin Oncol. 2005;23:676–684. - PubMed
-
- O'Connor OA, Portlock C, Moskowitz C, Hamlin P, Straus D, Gerecitano J, et al. Time to treatment response in patients with follicular lymphoma treated with bortezomib is longer compared with other histologic subtypes. Clin Cancer Res. 2010;16:719–726. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
