

The Effect of Age, Parity and Body Mass Index on the Efficacy, Safety, Placement and User Satisfaction Associated With Two Low-Dose Levonorgestrel Intrauterine Contraceptive Systems: Subgroup Analyses of Data From a Phase III Trial
- PMID: 26378938
- PMCID: PMC4574776
- DOI: 10.1371/journal.pone.0135309
The Effect of Age, Parity and Body Mass Index on the Efficacy, Safety, Placement and User Satisfaction Associated With Two Low-Dose Levonorgestrel Intrauterine Contraceptive Systems: Subgroup Analyses of Data From a Phase III Trial
Abstract
Objective: Two low-dose levonorgestrel intrauterine contraceptive systems (LNG-IUSs; total content 13.5 mg [average approx. 8 μg/24 hours over the first year; LNG-IUS 8] and total content 19.5 mg [average approx. 13 μg/24 hours over the first year; LNG-IUS 13]) have previously been shown to be highly effective (3-year Pearl Indices: 0.33 and 0.31, respectively), safe and well tolerated. The present subgroup analyses evaluated whether or not outcomes were affected by parity, age (18-25 vs 26-35 years), or body mass index (BMI, <30 vs ≥30 kg/m2).
Methods: Nulliparous and parous women aged 18‒35 years with regular menstrual cycles (21‒35 days) requesting contraception were randomized to 3 years of LNG-IUS 8 or LNG-IUS 13 use.
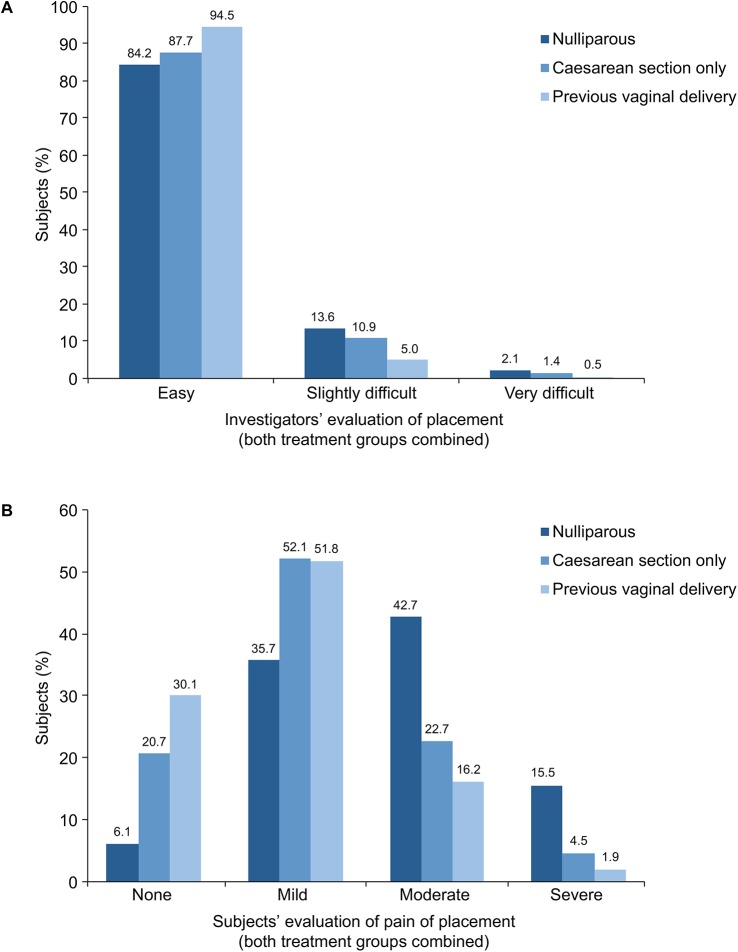
Results: In the LNG-IUS 8 and LNG-IUS 13 groups, 1432 and 1452 women, respectively, had a placement attempted and were included in the full analysis set; 39.2%, 39.2% and 17.1% were 18-25 years old, nulliparous and had a BMI ≥30 kg/m2, respectively. Both systems were similarly effective regardless of age, parity or BMI; the subgroup Pearl Indices had widely overlapping 95% confidence intervals. Placement of LNG-IUS 8 and LNG-IUS 13 was easier (p < 0.0001) and less painful (p < 0.0001) in women who had delivered vaginally than in women who had not. The complete/partial expulsion rate was 2.2-4.2% across all age and parity subgroups and higher in parous than in nulliparous women (p = 0.004). The incidence of pelvic inflammatory disease was 0.1-0.6% across all age and parity subgroups: nulliparous and younger women were not at higher risk than parous and older women, respectively. The ectopic pregnancy rate was 0.3-0.4% across all age and parity subgroups. Across all age and parity subgroups, the 3-year completion rate was 50.9-61.3% for LNG-IUS 8 and 57.9-61.1% for LNG-IUS 13, and was higher (p = 0.0001) among older than younger women in the LNG-IUS 8 group only.
Conclusions: LNG-IUS 8 and LNG-IUS 13 were highly effective, safe and well tolerated regardless of age or parity.
Trial registration: Clinical trials.gov NCT00528112.
Conflict of interest statement
Figures
Similar articles
-
Evaluation of a new, low-dose levonorgestrel intrauterine contraceptive system over 5 years of use.Eur J Obstet Gynecol Reprod Biol. 2017 Mar;210:22-28. doi: 10.1016/j.ejogrb.2016.11.022. Epub 2016 Nov 20. Eur J Obstet Gynecol Reprod Biol. 2017. PMID: 27930941 Clinical Trial.
-
A Phase III, single-arm study of LNG-IUS 8, a low-dose levonorgestrel intrauterine contraceptive system (total content 13.5mg) in postmenarcheal adolescents.Contraception. 2016 Jun;93(6):507-12. doi: 10.1016/j.contraception.2016.02.004. Epub 2016 Feb 9. Contraception. 2016. PMID: 26872720 Clinical Trial.
-
A single-arm phase III study exploring the efficacy and safety of LNG-IUS 8, a low-dose levonorgestrel intrauterine contraceptive system (total content 13.5 mg), in an Asia-Pacific population.Contraception. 2017 Apr;95(4):371-377. doi: 10.1016/j.contraception.2016.11.005. Epub 2016 Nov 29. Contraception. 2017. PMID: 27913229 Clinical Trial.
-
The levonorgestrel intrauterine system in nulliparous women.Contraception. 2007 Jun;75(6 Suppl):S12-5. doi: 10.1016/j.contraception.2007.01.018. Epub 2007 Apr 3. Contraception. 2007. PMID: 17531602 Review.
-
Levonorgestrel-releasing intrauterine system (LNG-IUS 12) for prevention of pregnancy for up to five years.Expert Rev Clin Pharmacol. 2017 Aug;10(8):833-842. doi: 10.1080/17512433.2017.1341308. Epub 2017 Jun 19. Expert Rev Clin Pharmacol. 2017. PMID: 28617060 Review.
Cited by
-
One-year follow up of contraceptive use and pregnancy rates after early medical abortion: Secondary outcomes from a randomized controlled trial of immediate post-abortion placement of intrauterine devices.Acta Obstet Gynecol Scand. 2023 Dec;102(12):1694-1702. doi: 10.1111/aogs.14662. Epub 2023 Aug 23. Acta Obstet Gynecol Scand. 2023. PMID: 37614066 Free PMC article. Clinical Trial.
-
Discontinuation rates of intrauterine contraception due to unfavourable bleeding: a systematic review.BMC Womens Health. 2022 Mar 21;22(1):82. doi: 10.1186/s12905-022-01657-6. BMC Womens Health. 2022. PMID: 35313863 Free PMC article.
-
The use of LNG-IUS-19.5 mg in daily gynecological routine practice in Germany: data from the Kyleena™ Satisfaction Study (KYSS).Arch Gynecol Obstet. 2024 May;309(5):2021-2030. doi: 10.1007/s00404-024-07421-5. Epub 2024 Feb 29. Arch Gynecol Obstet. 2024. PMID: 38421421 Free PMC article.
-
Hormonal contraceptives for contraception in overweight or obese women.Cochrane Database Syst Rev. 2016 Aug 18;2016(8):CD008452. doi: 10.1002/14651858.CD008452.pub4. Cochrane Database Syst Rev. 2016. PMID: 27537097 Free PMC article. Review.
-
Digital Medical Device Companion (MyIUS) for New Users of Intrauterine Systems: App Development Study.JMIR Med Inform. 2021 Jul 13;9(7):e24633. doi: 10.2196/24633. JMIR Med Inform. 2021. PMID: 34255688 Free PMC article.
References
-
- World Health Organization (2010) Medical eligibility criteria for contraceptive use: fourth edition. Available: http://whqlibdoc.who.int/publications/2010/9789241563888_eng.pdf. Accessed 11 May 2015.
-
- Centers for Disease Control and Prevention (2010) MMWR: Sexually transmitted diseases treatment guidelines 2010. Available: http://www.cdc.gov/std/treatment/2010/pid.htm. Accessed 21 October 2014.
-
- Faculty of the Royal College of Obstetricians and Gynaecologists (2009) UK medical eligibility for contraceptive use. Available: http://www.fsrh.org/pdfs/UKMEC2009.pdf. Accessed 27 July 2015.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
