

CTLA-4 Blockade Synergizes Therapeutically with PARP Inhibition in BRCA1-Deficient Ovarian Cancer
- PMID: 26138335
- PMCID: PMC4984269
- DOI: 10.1158/2326-6066.CIR-15-0044
CTLA-4 Blockade Synergizes Therapeutically with PARP Inhibition in BRCA1-Deficient Ovarian Cancer
Abstract
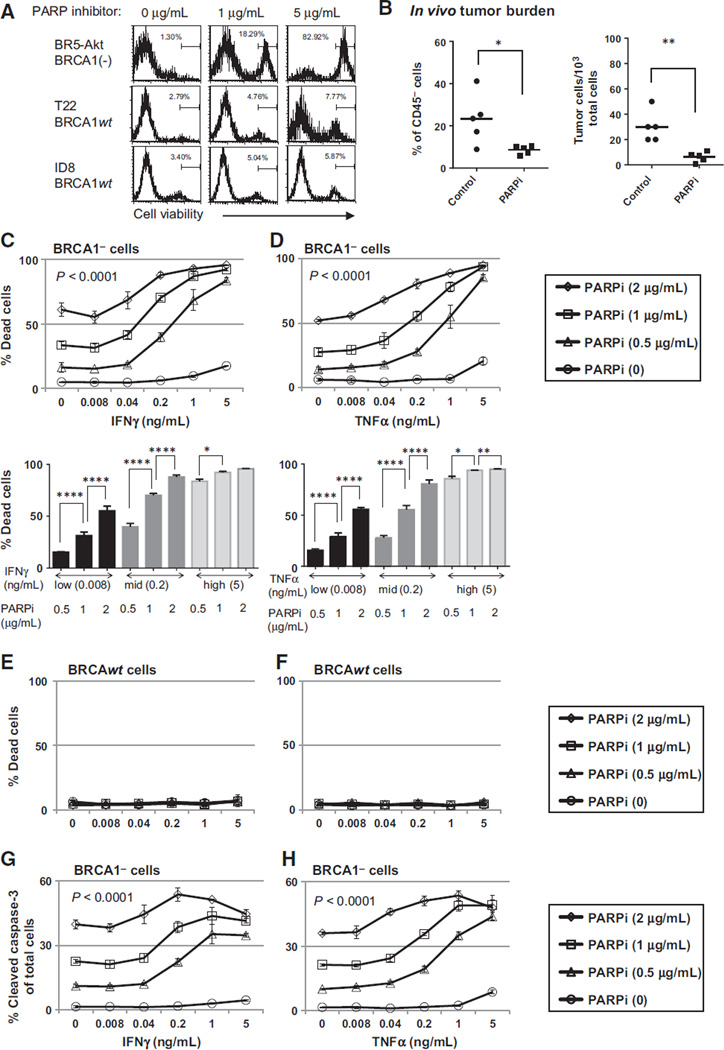
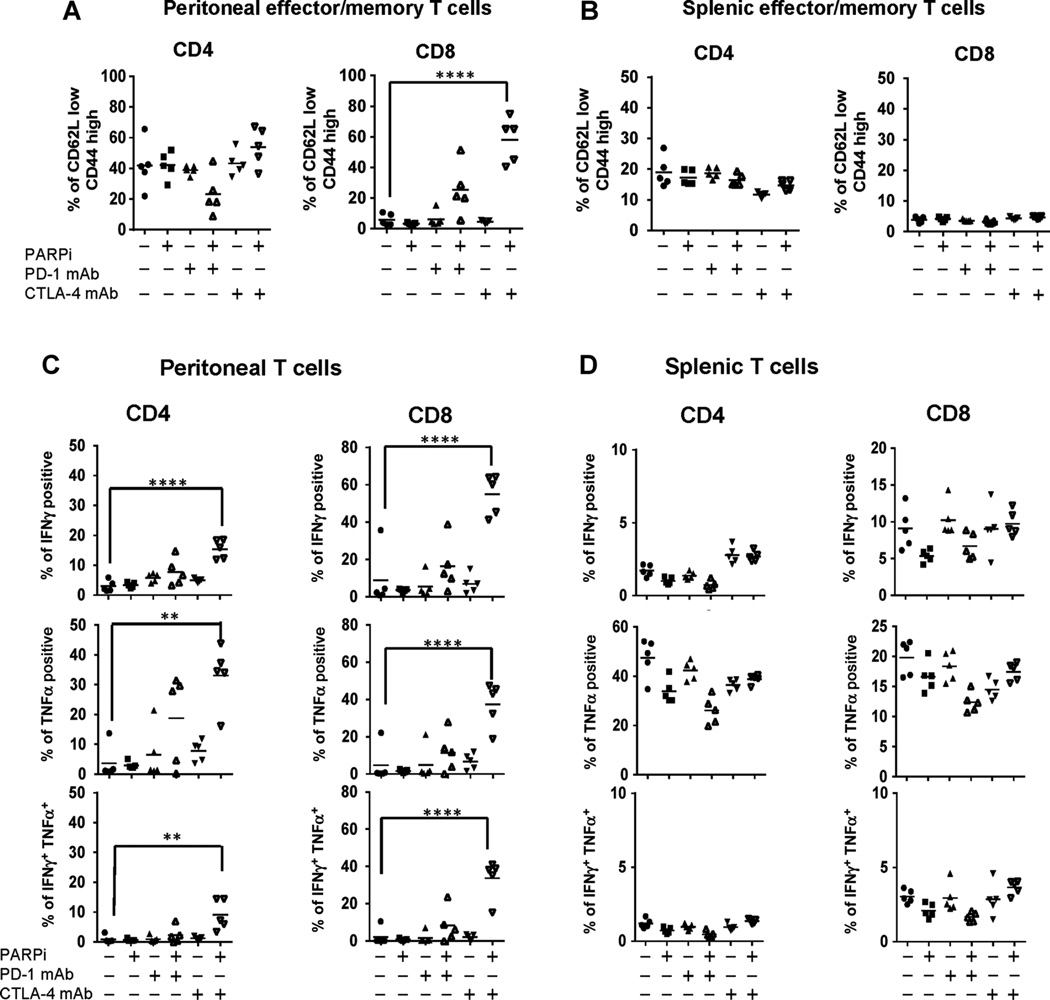
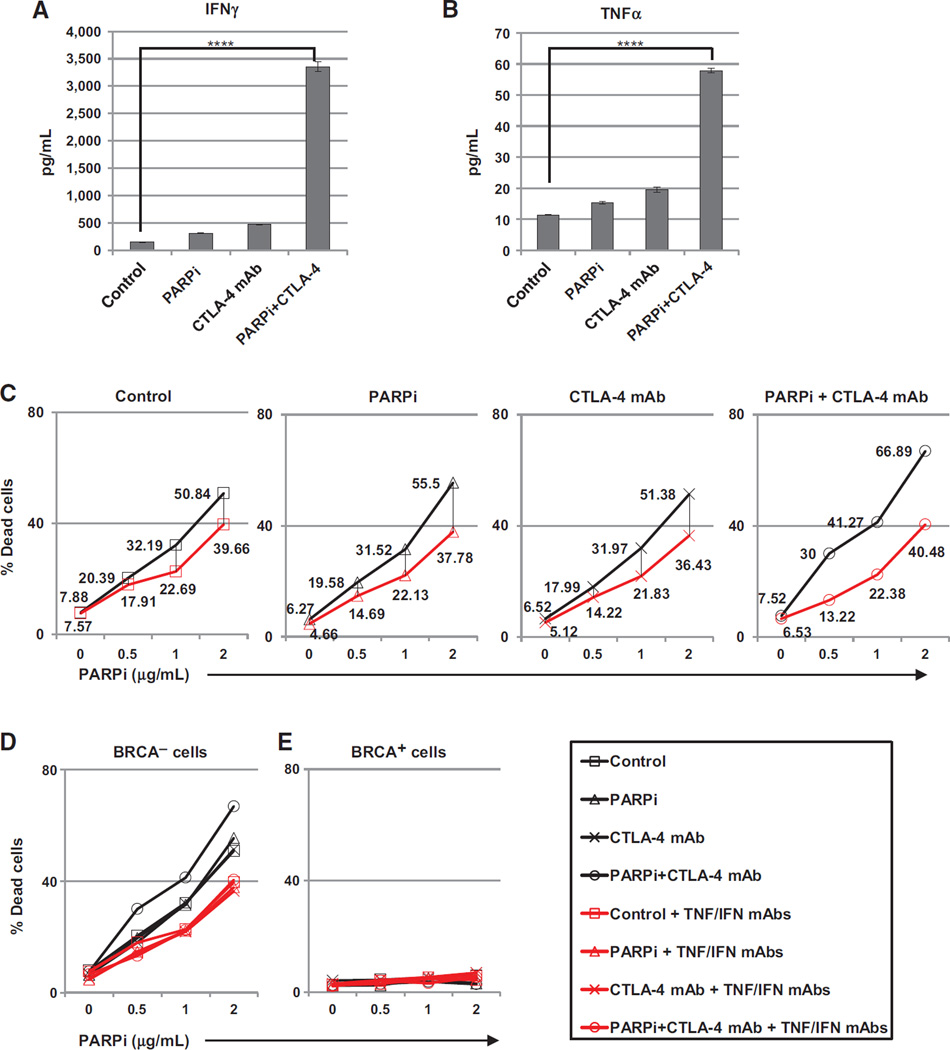
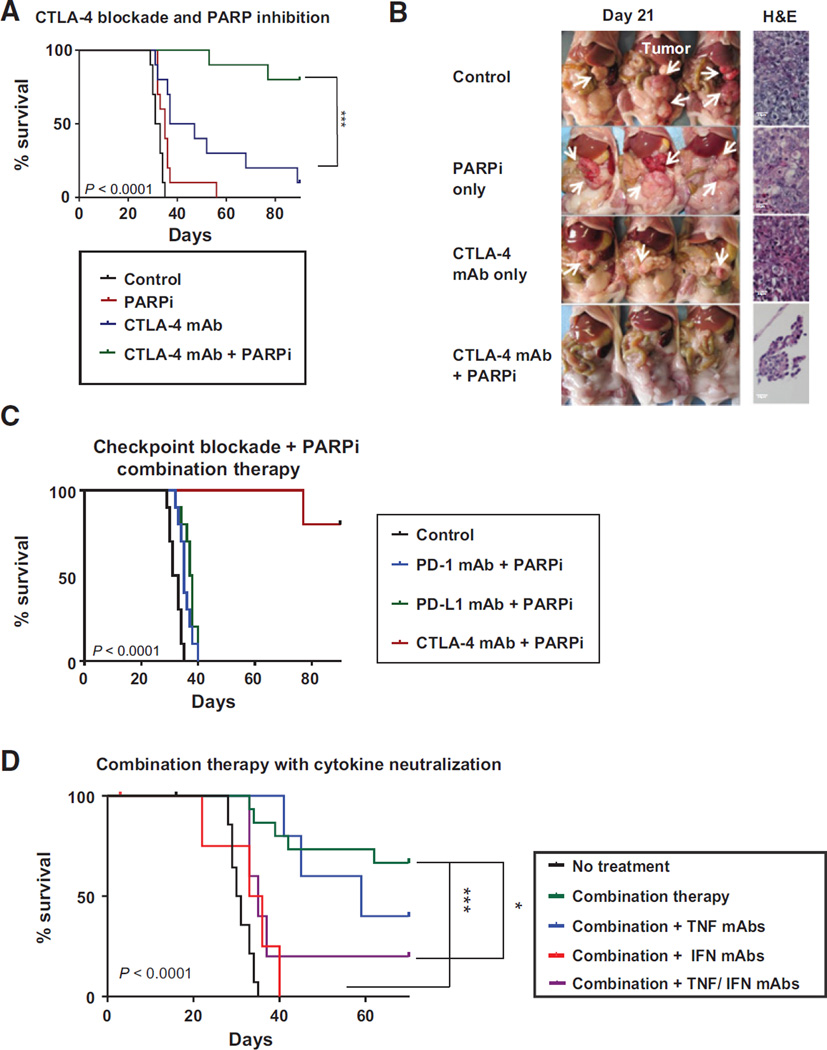
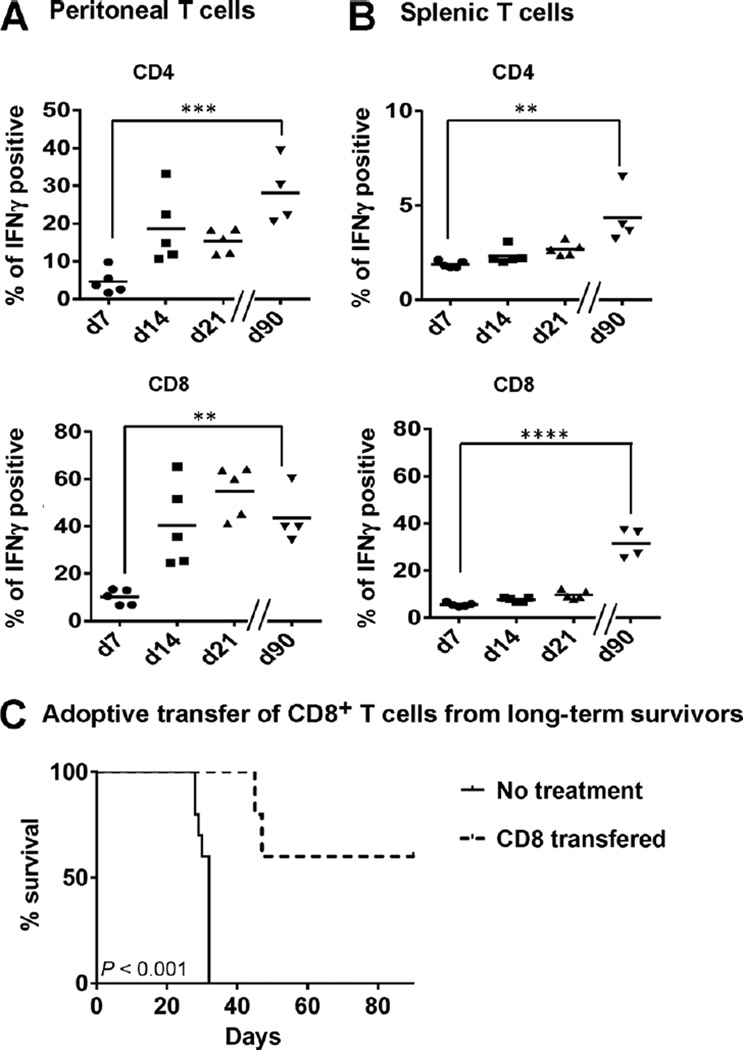
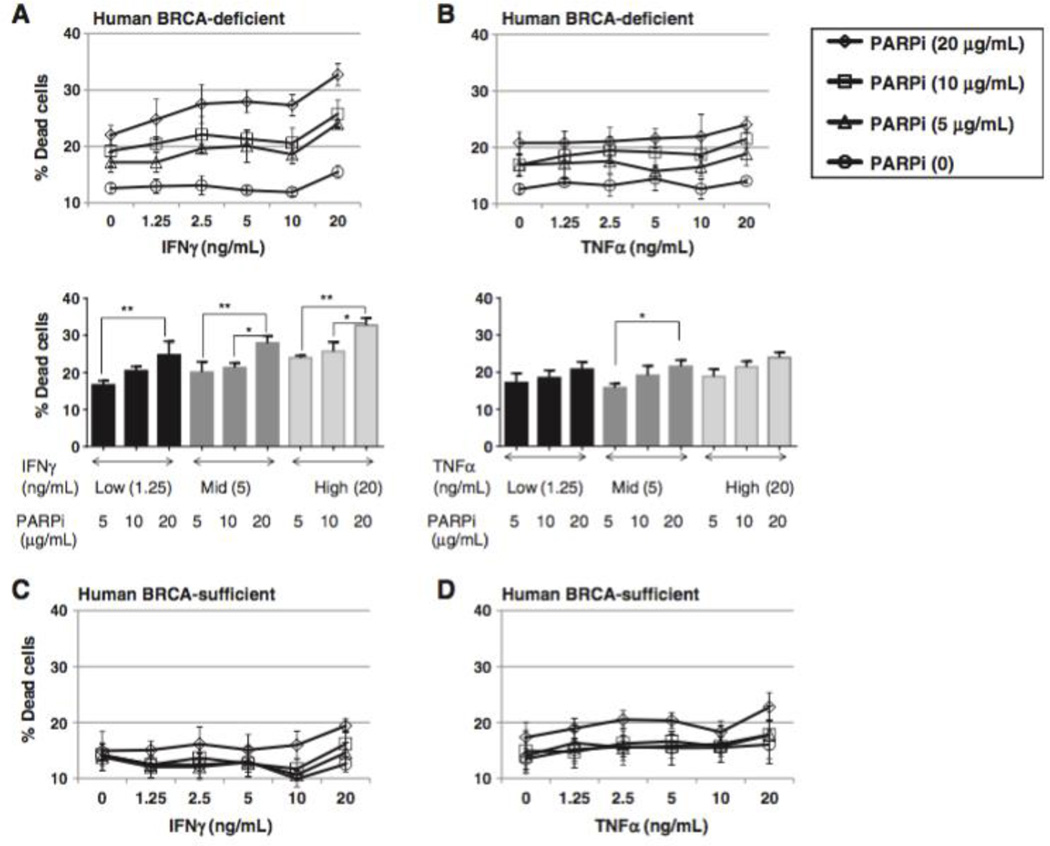
Immune checkpoint blockade has shown significant therapeutic efficacy in melanoma and other solid tumors, but results in ovarian cancer have been limited. With evidence that tumor immunogenicity modulates the response to checkpoint blockade, and data indicating that BRCA-deficient ovarian cancers express higher levels of immune response genes, we hypothesized that BRCA(-) ovarian tumors would be vulnerable to checkpoint blockade. To test this hypothesis, we used an immunocompetent BRCA1-deficient murine ovarian cancer model to compare treatment with CTLA-4 or PD-1/PD-L1 antibodies alone or combined with targeted cytotoxic therapy using a PARP inhibitor. Correlative studies were performed in vitro using human BRCA1(-) cells. We found that CTLA-4 antibody, but not PD-1/PD-L1 blockade, synergized therapeutically with the PARP inhibitor, resulting in immune-mediated tumor clearance and long-term survival in a majority of animals (P < 0.0001). The survival benefit of this combination was T-cell mediated and dependent on increases in local IFNγ production in the peritoneal tumor environment. Evidence of protective immune memory was observed more than 60 days after completion of therapy. Similar increases in the cytotoxic effect of PARP inhibition in the presence of elevated levels of IFNγ in human BRCA1(-) cancer cells support the translational potential of this treatment protocol. These results demonstrate that CTLA-4 blockade combined with PARP inhibition induces protective antitumor immunity and significant survival benefit in the BRCA1(-) tumor model, and support clinical testing of this regimen to improve outcomes for women with hereditary ovarian cancer.
©2015 American Association for Cancer Research.
Conflict of interest statement
No potential conflicts of interest were disclosed.
Figures
Similar articles
-
Decitabine Enhances Lymphocyte Migration and Function and Synergizes with CTLA-4 Blockade in a Murine Ovarian Cancer Model.Cancer Immunol Res. 2015 Sep;3(9):1030-41. doi: 10.1158/2326-6066.CIR-15-0073. Epub 2015 Jun 8. Cancer Immunol Res. 2015. PMID: 26056145
-
Synergistic effects of the immune checkpoint inhibitor CTLA-4 combined with the growth inhibitor lycorine in a mouse model of renal cell carcinoma.Oncotarget. 2017 Mar 28;8(13):21177-21186. doi: 10.18632/oncotarget.15505. Oncotarget. 2017. PMID: 28416753 Free PMC article.
-
Combined Radiation Therapy and Immune Checkpoint Blockade Therapy for Breast Cancer.Int J Radiat Oncol Biol Phys. 2017 Sep 1;99(1):153-164. doi: 10.1016/j.ijrobp.2017.05.029. Epub 2017 May 26. Int J Radiat Oncol Biol Phys. 2017. PMID: 28816141 Review.
-
Poxvirus-based active immunotherapy synergizes with CTLA-4 blockade to increase survival in a murine tumor model by improving the magnitude and quality of cytotoxic T cells.Cancer Immunol Immunother. 2016 May;65(5):537-49. doi: 10.1007/s00262-016-1816-7. Epub 2016 Mar 10. Cancer Immunol Immunother. 2016. PMID: 26961085 Free PMC article.
-
Immunotherapy for the treatment of breast cancer: checkpoint blockade, cancer vaccines, and future directions in combination immunotherapy.Clin Adv Hematol Oncol. 2016 Nov;14(11):922-933. Clin Adv Hematol Oncol. 2016. PMID: 27930644 Review.
Cited by
-
PARP inhibitor resistance in breast and gynecological cancer: Resistance mechanisms and combination therapy strategies.Front Pharmacol. 2022 Aug 25;13:967633. doi: 10.3389/fphar.2022.967633. eCollection 2022. Front Pharmacol. 2022. PMID: 36091750 Free PMC article. Review.
-
Update on Poly-ADP-ribose polymerase inhibition for ovarian cancer treatment.J Transl Med. 2016 Sep 15;14:267. doi: 10.1186/s12967-016-1027-1. J Transl Med. 2016. PMID: 27634150 Free PMC article. Review.
-
Phase I study of peposertib and avelumab with or without palliative radiotherapy in patients with advanced solid tumors.ESMO Open. 2024 Feb;9(2):102217. doi: 10.1016/j.esmoop.2023.102217. Epub 2024 Feb 5. ESMO Open. 2024. PMID: 38320431 Free PMC article. Clinical Trial.
-
The Synergistic Effect of PARP Inhibitors and Immune Checkpoint Inhibitors.Clin Med Insights Oncol. 2021 Feb 25;15:1179554921996288. doi: 10.1177/1179554921996288. eCollection 2021. Clin Med Insights Oncol. 2021. PMID: 33737855 Free PMC article. Review.
-
Combining PARP Inhibition and Immunotherapy in BRCA-Associated Cancers.Cancer Treat Res. 2023;186:207-221. doi: 10.1007/978-3-031-30065-3_12. Cancer Treat Res. 2023. PMID: 37978138
References
-
- Yang YF, Zou JP, Mu J, Wijesuriya R, Ono S, Walunas T, et al. Enhanced induction of antitumor T-cell responses by cytotoxic T lymphocyte-associated molecule-4 blockade: the effect is manifested only at the restricted tumor-bearing stages. Cancer Res. 1997;57:4036–4041. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
