

Healthcare utilization and costs associated with S. aureus and P. aeruginosa pneumonia in the intensive care unit: a retrospective observational cohort study in a US claims database
- PMID: 26093384
- PMCID: PMC4475310
- DOI: 10.1186/s12913-015-0917-x
Healthcare utilization and costs associated with S. aureus and P. aeruginosa pneumonia in the intensive care unit: a retrospective observational cohort study in a US claims database
Abstract
Background: Staphylococcus aureus and Pseudomonas aeruginosa are major causes of pneumonia in intensive care unit (ICU) patients. Limited data exist regarding the health economic impact of S. aureus and P. aeruginosa pneumonias in the ICU setting.
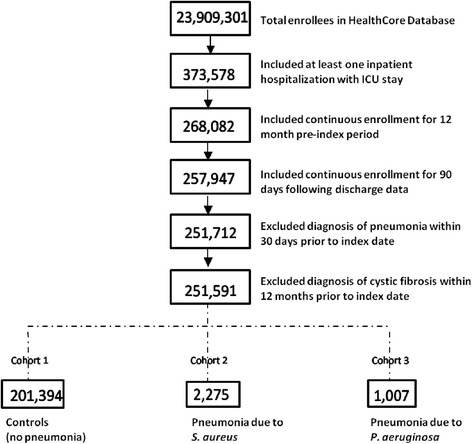
Methods: We conducted a retrospective observational cohort study using a 29.6 million enrollee US medical and pharmacy administrative claims database. ICU patients with S. aureus or P. aeruginosa infection per International Classification of Diseases, 9th ed. coding between 01/01/2007-8/31/2012 were compared with ICU patients without any pneumonia or infections of interest. Primary outcomes were costs in 2012 US dollars, healthcare utilization and all-cause mortality associated with hospital-acquired S. aureus or P. aeruginosa pneumonia, and the relative odds of incurring higher costs due to a comorbid condition.
Results: Patients with S. aureus or P. aeruginosa pneumonia had longer mean hospital (37.9 or 55.4 vs 7.2 days, P < .001) and ICU stays (6.9 or 14.8 vs 1.1 days, P < .001), a higher rate of mechanical ventilation (62.6 % or 62.3 % vs 7.4 %, P < .001), higher mortality (16.0 % or 20.2 % vs 3.1 %, P < .001), and higher total mean hospitalization costs ($146,978 or $213,104 vs $33,851, P < .001) vs controls. Pneumonia survivors had significantly increased risk of rehospitalization within 30 days (27.2 % or 31.1 % vs 15.3 %, P < .001). Comorbid conditions were not associated with increased cost in the pneumonia cohorts.
Conclusions: Healthcare costs and resource utilization were high among ICU patients with S. aureus or P. aeruginosa pneumonia. Reducing the incidence of these infections could lead to substantial cost savings in the United States.
Figures
Similar articles
-
Outcome and attributable cost of ventilator-associated pneumonia among intensive care unit patients in a suburban medical center.Crit Care Med. 2003 May;31(5):1312-7. doi: 10.1097/01.CCM.0000063087.93157.06. Crit Care Med. 2003. PMID: 12771596
-
Rationale and design of ASPIRE-ICU: a prospective cohort study on the incidence and predictors of Staphylococcus aureus and Pseudomonas aeruginosa pneumonia in the ICU.BMC Infect Dis. 2017 Sep 25;17(1):643. doi: 10.1186/s12879-017-2739-4. BMC Infect Dis. 2017. PMID: 28946849 Free PMC article.
-
[Impact on morbidity and costs of methicillin-resistant Staphylococcus aureus nosocomial pneumonia in intensive care patients].Presse Med. 2009 Jan;38(1):25-33. doi: 10.1016/j.lpm.2008.06.005. Epub 2008 Sep 3. Presse Med. 2009. PMID: 18771897 French.
-
Disease burden of intensive care unit-acquired pneumonia in China: a systematic review and meta-analysis.Int J Infect Dis. 2014 Dec;29:84-90. doi: 10.1016/j.ijid.2014.05.030. Epub 2014 Oct 24. Int J Infect Dis. 2014. PMID: 25449241 Review.
-
Reducing costs and patient morbidity in the enterally fed intensive care unit patient.JPEN J Parenter Enteral Nutr. 2005 Jan-Feb;29(1 Suppl):S62-9. doi: 10.1177/01486071050290S1S62. JPEN J Parenter Enteral Nutr. 2005. PMID: 15709547 Review.
Cited by
-
Fast-track extubation in patients after intracranial hematoma surgery.Exp Ther Med. 2020 Apr;19(4):2563-2569. doi: 10.3892/etm.2020.8507. Epub 2020 Feb 10. Exp Ther Med. 2020. PMID: 32256735 Free PMC article.
-
Experimental phage therapy against haematogenous multi-drug resistant Staphylococcus aureus pneumonia in mice.Afr J Lab Med. 2016 Sep 30;5(1):435. doi: 10.4102/ajlm.v5i1.435. eCollection 2016. Afr J Lab Med. 2016. PMID: 28879116 Free PMC article.
-
Antibacterial and antibiofilm potentials of vancomycin-loaded niosomal drug delivery system against methicillin-resistant Staphylococcus aureus (MRSA) infections.BMC Biotechnol. 2024 Jul 8;24(1):47. doi: 10.1186/s12896-024-00874-1. BMC Biotechnol. 2024. PMID: 38978013 Free PMC article.
-
Opportunistic Pathogens in Drinking Water Distribution Systems-A Review.Microorganisms. 2024 Apr 30;12(5):916. doi: 10.3390/microorganisms12050916. Microorganisms. 2024. PMID: 38792751 Free PMC article. Review.
-
Antimicrobial approaches in the prevention of Staphylococcus aureus infections: a review.J Antimicrob Chemother. 2019 Feb 1;74(2):281-294. doi: 10.1093/jac/dky421. J Antimicrob Chemother. 2019. PMID: 30376041 Free PMC article. Review.
References
-
- Esperatti M, Ferrer M, Theessen A, Liapikou A, Valencia M, Saucedo LM, Zavala E, Welte T, Torres A. Nosocomial pneumonia in the intensive care unit acquired by mechanically ventilated versus nonventilated patients. Am J Respir Crit Care Med. 2010;182:1533–1539. doi: 10.1164/rccm.201001-0094OC. - DOI - PubMed
-
- Park DR. The microbiology of ventilator-assisted pneumonia. Resp Care. 2005;50:742–765. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
