

Abnormal right ventricular relaxation in pulmonary hypertension
- PMID: 26064464
- PMCID: PMC4449250
- DOI: 10.1086/681268
Abnormal right ventricular relaxation in pulmonary hypertension
Abstract
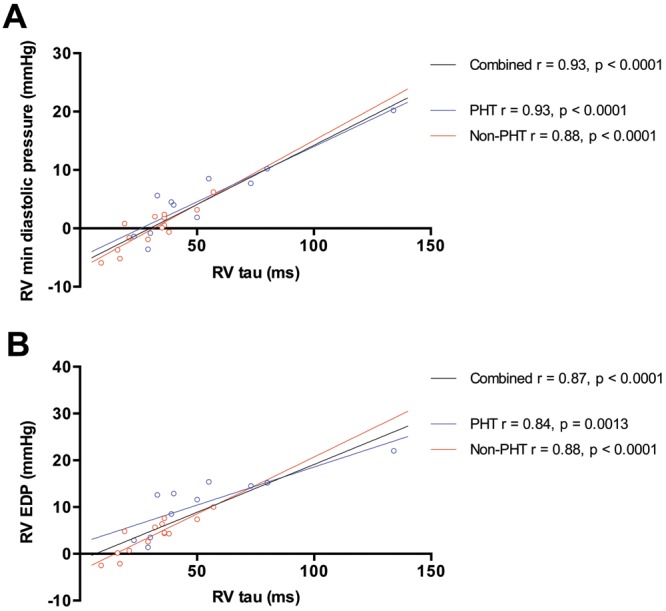
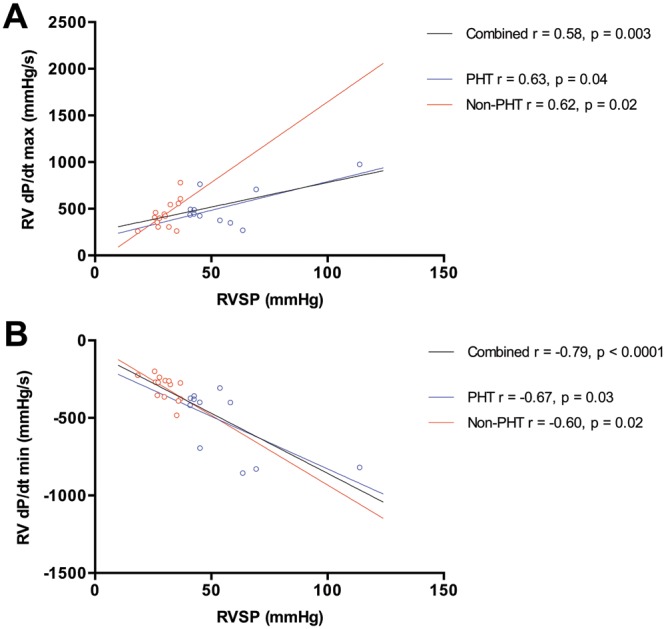
Left ventricular diastolic dysfunction is a well-described complication of systemic hypertension. However, less is known regarding the effect of chronic pressure overload on right ventricular (RV) diastolic function. We hypothesized that pulmonary hypertension (PHT) is associated with abnormal RV early relaxation and that this would be best shown by invasive pressure measurement. Twenty-five patients undergoing right heart catheterization for investigation of breathlessness and/or suspected PHT were studied. In addition to standard measurements, RV pressure was sampled with a high-fidelity micromanometer, and RV pressure/time curves were analyzed. Patients were divided into a PHT group and a non-PHT group on the basis of a derived mean pulmonary artery systolic pressure of 25 mmHg. Eleven patients were classified to the PHT group. This group had significantly higher RV minimum diastolic pressure ([Formula: see text] vs. [Formula: see text] mmHg, [Formula: see text]) and RV end-diastolic pressure (RVEDP; [Formula: see text] vs. [Formula: see text] mmHg, [Formula: see text]), and RV τ was significantly prolonged ([Formula: see text] vs. [Formula: see text] ms, [Formula: see text]). There were strong correlations between RV τ and RV minimum diastolic pressure ([Formula: see text], [Formula: see text]) and between RV τ and RVEDP ([Formula: see text], [Formula: see text]). There was a trend toward increased RV contractility (end-systolic elastance) in the PHT group ([Formula: see text] vs. [Formula: see text] mmHg/mL, [Formula: see text]) and a correlation between RV systolic pressure and first derivative of maximum pressure change ([Formula: see text], [Formula: see text]). Stroke volumes were similar. Invasive measures of RV early relaxation are abnormal in patients with PHT, whereas measured contractility is static or increasing, which suggests that diastolic dysfunction may precede systolic dysfunction. Furthermore, there is a strong association between measures of RV relaxation and RV filling pressures.
Keywords: diastolic function; heart failure; pulmonary hypertension; right ventricle; right ventricular function.
Figures
Similar articles
-
Right ventricular diastolic dysfunction in heart failure.Circulation. 1996 Apr 15;93(8):1509-14. doi: 10.1161/01.cir.93.8.1509. Circulation. 1996. PMID: 8608618
-
Right and left ventricular interaction in pulmonary hypertension: Insight from velocity vector imaging.Echocardiography. 2019 May;36(5):877-887. doi: 10.1111/echo.14328. Epub 2019 Apr 15. Echocardiography. 2019. PMID: 30985965
-
[Effects of maintenance hemodialysis on right ventricular dysfunction in patients with end-stage renal disease].Sichuan Da Xue Xue Bao Yi Xue Ban. 2014 Sep;45(5):814-8. Sichuan Da Xue Xue Bao Yi Xue Ban. 2014. PMID: 25341347 Chinese.
-
Clinical aspects of left ventricular diastolic function assessed by Doppler echocardiography following acute myocardial infarction.Dan Med Bull. 2001 Nov;48(4):199-210. Dan Med Bull. 2001. PMID: 11767125 Review.
-
The right ventricle: interaction with the pulmonary circulation.Crit Care. 2016 Sep 10;20(1):266. doi: 10.1186/s13054-016-1440-0. Crit Care. 2016. PMID: 27613549 Free PMC article. Review.
Cited by
-
Right atrial-right ventricular coupling in heart failure with preserved ejection fraction.Clin Res Cardiol. 2020 Jan;109(1):54-66. doi: 10.1007/s00392-019-01484-0. Epub 2019 May 3. Clin Res Cardiol. 2020. PMID: 31053957
-
Right ventricular diastolic dysfunction and failure: a review.Heart Fail Rev. 2022 Jul;27(4):1077-1090. doi: 10.1007/s10741-021-10123-8. Epub 2021 May 19. Heart Fail Rev. 2022. PMID: 34013436 Review.
-
A novel index equivalent to the myocardial performance index for right ventricular functional assessment in children and adolescent patients.Sci Rep. 2019 Dec 27;9(1):19975. doi: 10.1038/s41598-019-56564-y. Sci Rep. 2019. PMID: 31882794 Free PMC article.
-
Accuracy of Swan‒Ganz catheterization-based assessment of right ventricular function: Validation study using high-fidelity micromanometry-derived values as reference.Pulm Circ. 2022 Apr 18;12(2):e12078. doi: 10.1002/pul2.12078. eCollection 2022 Apr. Pulm Circ. 2022. PMID: 35514782 Free PMC article.
-
Clinical Determinants and Prognostic Implications of Right Ventricular Dysfunction in Pulmonary Hypertension Caused by Chronic Lung Disease.J Am Heart Assoc. 2019 Jan 22;8(2):e011464. doi: 10.1161/JAHA.118.011464. J Am Heart Assoc. 2019. PMID: 30646788 Free PMC article.
References
-
- Aurigemma GP, Gaasch WH. Diastolic heart failure. N Engl J Med 2004;351(11):1097–1105. - PubMed
-
- Hay I, Rich J, Ferber P, Burkhoff D, Maurer MS. Role of impaired myocardial relaxation in the production of elevated left ventricular filling pressure. Am J Physiol Heart Circ Physiol 2005;288(3):H1203–H1208. - PubMed
-
- La Gerche A, Heidbüchel H, Burns AT, et al. Disproportionate exercise load and remodeling of the athlete’s right ventricle. Med Sci Sports Exerc 2011;43(6):974–981. - PubMed
-
- Champion HC, Michelakis ED, Hassoun PM. Comprehensive invasive and noninvasive approach to the right ventricle-pulmonary circulation unit: state of the art and clinical and research implications. Circulation 2009;120(11):992–1007. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
