

HIV Infection Is Associated With Progression of Subclinical Carotid Atherosclerosis
- PMID: 25904369
- PMCID: PMC4607734
- DOI: 10.1093/cid/civ325
HIV Infection Is Associated With Progression of Subclinical Carotid Atherosclerosis
Abstract
Background: Individuals infected with human immunodeficiency virus (HIV) live longer as a result of effective treatment, but long-term consequences of infection, treatment, and immunological dysfunction are poorly understood.
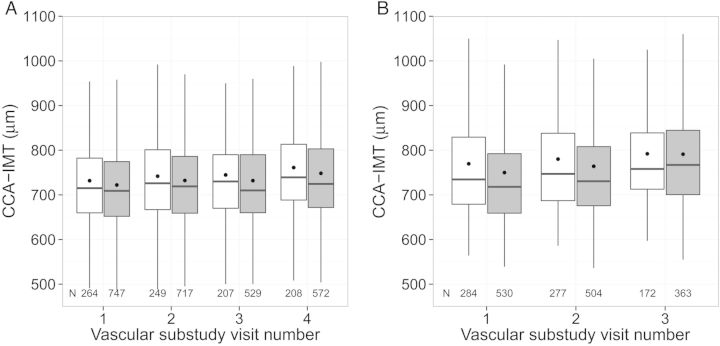
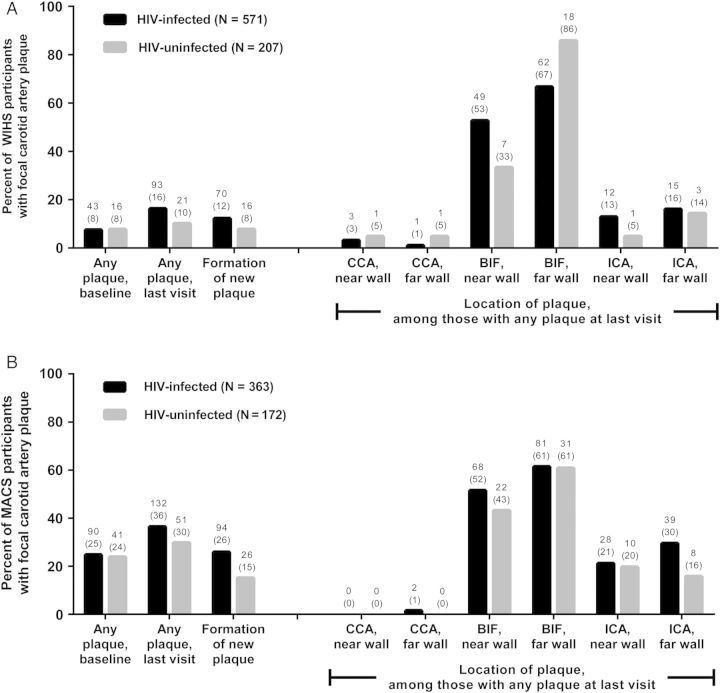
Methods: We prospectively examined 1011 women (74% HIV-infected) in the Women's Interagency HIV Study and 811 men (65% HIV-infected) in the Multicenter AIDS Cohort Study who underwent repeated B-mode carotid artery ultrasound imaging in 2004-2013. Outcomes included changes in right common carotid artery intima-media thickness (CCA-IMT) and new focal carotid artery plaque formation (IMT >1.5 mm) over median 7 years. We assessed the association between HIV serostatus and progression of subclinical atherosclerosis, adjusting for demographic, behavioral, and cardiometabolic risk factors.
Results: Unadjusted mean CCA-IMT increased (725 to 752 µm in women, 757 to 790 µm in men), but CCA-IMT progression did not differ by HIV serostatus, either in combined or sex-specific analyses. Focal plaque prevalence increased from 8% to 15% in women and 25% to 34% in men over 7 years. HIV-infected individuals had 1.6-fold greater risk of new plaque formation compared with HIV-uninfected individuals (relative risk [RR] 1.61, 95% CI, 1.12-2.32), adjusting for cardiometabolic factors; the association was similar by sex. Increased plaque occurred even among persistently virologically suppressed HIV-infected individuals compared with uninfected individuals (RR 1.56, 95% CI, 1.07-2.27). HIV-infected individuals with baseline CD4+ ≥ 500 cells/µL had plaque risk not statistically different from uninfected individuals.
Conclusions: HIV infection is associated with greater increases in focal plaque among women and men, potentially mediated by factors associated with immunodeficiency or HIV replication at levels below current limits of detection.
Keywords: HIV infection; atherosclerosis; cardiovascular disease; intima-media thickness; viral load.
© The Author 2015. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Carotid intima-media thickness is slightly increased over time in HIV-1-infected patients.HIV Med. 2005 Nov;6(6):380-7. doi: 10.1111/j.1468-1293.2005.00324.x. HIV Med. 2005. PMID: 16268819
-
Carotid atherosclerosis is a stronger predictor of myocardial infarction in women than in men: a 6-year follow-up study of 6226 persons: the Tromsø Study.Stroke. 2007 Nov;38(11):2873-80. doi: 10.1161/STROKEAHA.107.487264. Epub 2007 Sep 27. Stroke. 2007. PMID: 17901390
-
Progression of atherosclerosis as assessed by carotid intima-media thickness in patients with HIV infection.Circulation. 2004 Apr 6;109(13):1603-8. doi: 10.1161/01.CIR.0000124480.32233.8A. Epub 2004 Mar 15. Circulation. 2004. PMID: 15023877
-
[Carotid artery disease and human immunodeficiency virus (HIV) infection].Neurologia. 2009 Jun;24(5):318-30. Neurologia. 2009. PMID: 19642035 Review. Spanish.
-
HIV positivity, protease inhibitor exposure and subclinical atherosclerosis: a systematic review and meta-analysis of observational studies.Heart. 2009 Nov;95(22):1826-35. doi: 10.1136/hrt.2009.177774. Epub 2009 Jul 23. Heart. 2009. PMID: 19632982 Review.
Cited by
-
The effect of HIV infection, antiretroviral therapy on carotid intima-media thickness: A systematic review and meta-analysis.Life Sci. 2019 Oct 15;235:116851. doi: 10.1016/j.lfs.2019.116851. Epub 2019 Sep 6. Life Sci. 2019. PMID: 31499070 Free PMC article.
-
Gut Microbiota, Plasma Metabolomic Profiles, and Carotid Artery Atherosclerosis in HIV Infection.Arterioscler Thromb Vasc Biol. 2022 Aug;42(8):1081-1093. doi: 10.1161/ATVBAHA.121.317276. Epub 2022 Jun 9. Arterioscler Thromb Vasc Biol. 2022. PMID: 35678187 Free PMC article.
-
Sex Hormones, the Stool Microbiome, and Subclinical Atherosclerosis in Women With and Without HIV.J Clin Endocrinol Metab. 2024 Jan 18;109(2):483-497. doi: 10.1210/clinem/dgad510. J Clin Endocrinol Metab. 2024. PMID: 37643897 Free PMC article.
-
Characteristics, Prevention, and Management of Cardiovascular Disease in People Living With HIV: A Scientific Statement From the American Heart Association.Circulation. 2019 Jul 9;140(2):e98-e124. doi: 10.1161/CIR.0000000000000695. Epub 2019 Jun 3. Circulation. 2019. PMID: 31154814 Free PMC article. Review.
-
Decreased Vigorous Physical Activity in School-Aged Children with Human Immunodeficiency Virus in Johannesburg, South Africa.J Pediatr. 2016 May;172:103-9. doi: 10.1016/j.jpeds.2016.01.034. Epub 2016 Feb 26. J Pediatr. 2016. PMID: 26922104 Free PMC article.
References
-
- Palella FJ, Jr, Delaney KM, Moorman AC, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med 1998; 338:853–60. - PubMed
-
- Wada N, Jacobson LP, Cohen M, French A, Phair J, Munoz A. Cause-specific life expectancies after 35 years of age for human immunodeficiency syndrome-infected and human immunodeficiency syndrome-negative individuals followed simultaneously in long-term cohort studies, 1984–2008. Am J Epidemiol 2013; 177:116–25. - PMC - PubMed
-
- Sackoff JE, Hanna DB, Pfeiffer MR, Torian LV. Causes of death among persons with AIDS in the era of highly active antiretroviral therapy: New York City. Ann Intern Med 2006; 145:397–406. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 AI035042/AI/NIAID NIH HHS/United States
- R01-HL-095140/HL/NHLBI NIH HHS/United States
- U01-AI-034994/AI/NIAID NIH HHS/United States
- U01 AI031834/AI/NIAID NIH HHS/United States
- UL1-TR000004/TR/NCATS NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- R01-HL-083760/HL/NHLBI NIH HHS/United States
- UL1-TR000454/TR/NCATS NIH HHS/United States
- R01 HL095140/HL/NHLBI NIH HHS/United States
- P30 AI051519/AI/NIAID NIH HHS/United States
- U01-AI-034993/AI/NIAID NIH HHS/United States
- R01-HL-095129/HL/NHLBI NIH HHS/United States
- U01-AI35040/AI/NIAID NIH HHS/United States
- R21 HL120394/HL/NHLBI NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- R01 HL126543/HL/NHLBI NIH HHS/United States
- R01 HL083760/HL/NHLBI NIH HHS/United States
- U01-AI-035004/AI/NIAID NIH HHS/United States
- U01-AI35042/AI/NIAID NIH HHS/United States
- U01 AI035041/AI/NIAID NIH HHS/United States
- UM1 AI035043/AI/NIAID NIH HHS/United States
- R21-HL-120394/HL/NHLBI NIH HHS/United States
- R01 HL095129/HL/NHLBI NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- UL1 TR001073/TR/NCATS NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- U01-AI35041/AI/NIAID NIH HHS/United States
- U01-AI35039/AI/NIAID NIH HHS/United States
- U01-AI-034989/AI/NIAID NIH HHS/United States
- U01-AI-042590/AI/NIAID NIH HHS/United States
- U01-HD-032632/HD/NICHD NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- UL1-TR000424/TR/NCATS NIH HHS/United States
- P30-AI-051519/AI/NIAID NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
- U01 AI035039/AI/NIAID NIH HHS/United States
- U01-AI-031834/AI/NIAID NIH HHS/United States
- UM1-AI35043/AI/NIAID NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
