

Functional disability and nursing resource use are predictive of antimicrobial resistance in nursing homes
- PMID: 25857440
- PMCID: PMC4406786
- DOI: 10.1111/jgs.13353
Functional disability and nursing resource use are predictive of antimicrobial resistance in nursing homes
Abstract
Objectives: To use a simple measure of activities of daily living, wounds, and indwelling devices (urinary catheter, feeding tube) to predict prevalent, new, and intermittent multidrug-resistant organism (MDRO) acquisition in nursing home (NH) residents.
Design: Secondary analysis, prospective cohort study.
Setting: Southeast Michigan NHs (n = 15).
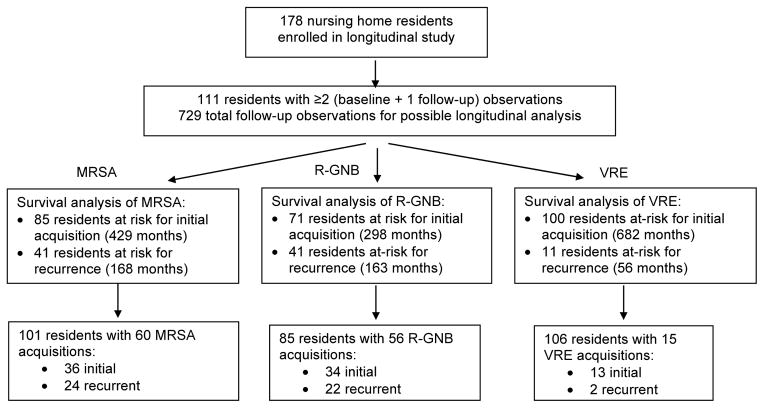
Participants: NH residents (N = 111, mean age 81) with two or more monthly visits (729 total).
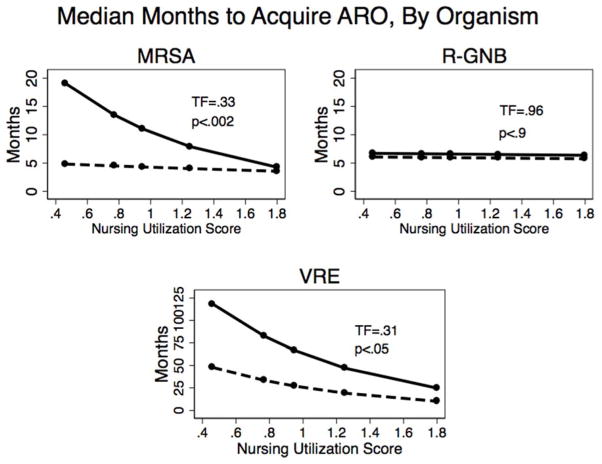
Measurements: Monthly microbiological surveillance for MDROs from multiple anatomic sites from enrollment until discharge or 1 year. The Arling scale, previously developed as a measure of NH residents' need (time-intensity) for nursing resources, was used to predict prevalent and time to new or intermittent acquisition (months) of methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), and antibiotic-resistant gram-negative bacteria (R-GNB) colonization using multiple-failure accelerated time-factor survival analysis, controlling for comorbidity, hospitalization, and antibiotic use in the prior month.
Results: One-fifth of participants had a wound, and one-third had a device. There were 60 acquisitions of MRSA, 56 of R-GNB, and 15 of VRE. Expected time to acquisition was less than 1 year for MRSA (median 6.7 months) and R-GNB (median 4.5 months) and more than 1 year for VRE (median 40 months). Arling score was associated with earlier new MRSA and VRE acquisition. A resident with only mild functional impairment and no device or wound would be expected to acquire MRSA in 20 months, versus 5 months for someone needing the most-intense nursing contact.
Conclusion: MDRO acquisition is common in community NHs. Need for nursing care predicts new MDRO acquisition in NHs, suggesting potential mechanisms for MDRO acquisition and strategies for future interventions for high-risk individuals (e.g., enhanced barrier precautions).
Keywords: functional disability; multidrug-resistant organisms; nursing homes.
Published 2015. This article is a U.S. Government work and is in the public domain in the USA.
Conflict of interest statement
[Table: see text]
Figures
Similar articles
-
A targeted infection prevention intervention in nursing home residents with indwelling devices: a randomized clinical trial.JAMA Intern Med. 2015 May;175(5):714-23. doi: 10.1001/jamainternmed.2015.132. JAMA Intern Med. 2015. PMID: 25775048 Free PMC article. Clinical Trial.
-
Longitudinal Assessment of Multidrug-Resistant Organisms in Newly Admitted Nursing Facility Patients: Implications for an Evolving Population.Clin Infect Dis. 2018 Aug 31;67(6):837-844. doi: 10.1093/cid/ciy194. Clin Infect Dis. 2018. PMID: 29635360 Free PMC article.
-
Methicillin-resistant Staphylococcus aureus: site of acquisition and strain variation in high-risk nursing home residents with indwelling devices.Infect Control Hosp Epidemiol. 2014 Dec;35(12):1458-65. doi: 10.1086/678599. Epub 2014 Nov 5. Infect Control Hosp Epidemiol. 2014. PMID: 25419767 Free PMC article.
-
Conceptual model for reducing infections and antimicrobial resistance in skilled nursing facilities: focusing on residents with indwelling devices.Clin Infect Dis. 2011 Mar 1;52(5):654-61. doi: 10.1093/cid/ciq205. Clin Infect Dis. 2011. PMID: 21292670 Free PMC article. Review.
-
Approaches to multidrug-resistant organism prevention and control in long-term care facilities for older people: a systematic review and meta-analysis.Antimicrob Resist Infect Control. 2022 Jan 15;11(1):7. doi: 10.1186/s13756-021-01044-0. Antimicrob Resist Infect Control. 2022. PMID: 35033198 Free PMC article. Review.
Cited by
-
Effectiveness of a Multicomponent Intervention to Reduce Multidrug-Resistant Organisms in Nursing Homes: A Cluster Randomized Clinical Trial.JAMA Netw Open. 2021 Jul 1;4(7):e2116555. doi: 10.1001/jamanetworkopen.2021.16555. JAMA Netw Open. 2021. PMID: 34269807 Free PMC article. Clinical Trial.
-
Reimagining Infection Control in U.S. Nursing Homes in the Era of COVID-19.J Am Med Dir Assoc. 2022 Dec;23(12):1909-1915. doi: 10.1016/j.jamda.2022.10.022. Epub 2022 Nov 16. J Am Med Dir Assoc. 2022. PMID: 36423677 Free PMC article.
-
Epidemiology of resistant gram-negative bacteria in nursing homes.Infect Control Hosp Epidemiol. 2023 Sep;44(9):1423-1428. doi: 10.1017/ice.2022.225. Epub 2023 Mar 14. Infect Control Hosp Epidemiol. 2023. PMID: 36916011 Free PMC article.
-
Predictors of methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci co-colonization among nursing facility patients.Am J Infect Control. 2019 Apr;47(4):415-420. doi: 10.1016/j.ajic.2018.09.026. Epub 2018 Nov 28. Am J Infect Control. 2019. PMID: 30502107 Free PMC article.
-
Prevalence and Risk Factors for Multidrug-Resistant Organisms Colonization in Long-Term Care Facilities Around the World: A Review.Antibiotics (Basel). 2021 Jun 7;10(6):680. doi: 10.3390/antibiotics10060680. Antibiotics (Basel). 2021. PMID: 34200238 Free PMC article. Review.
References
-
- Reynolds C, Quan V, Kim D, et al. Methicillin-resistant Staphylococcus aureus (MRSA) carriage in 10 nursing homes in Orange County, California. Infect Control Hosp Epidemiol. 2011;32:91–93. - PubMed
-
- Jain R, Kralovic SM, Evans ME, et al. Veterans Affairs initiative to prevent methicillin-resistant Staphylococcus aureus infections. N Engl J Med. 2011;364:1419–1430. - PubMed
-
- Bonomo RA. Multiple antibiotic-resistant bacteria in long-term-care facilities: An emerging problem in the practice of infectious diseases. Clin Infect Dis. 2000;31:1414–1422. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
