

Annual Report to the Nation on the Status of Cancer, 1975-2011, Featuring Incidence of Breast Cancer Subtypes by Race/Ethnicity, Poverty, and State
- PMID: 25825511
- PMCID: PMC4603551
- DOI: 10.1093/jnci/djv048
Annual Report to the Nation on the Status of Cancer, 1975-2011, Featuring Incidence of Breast Cancer Subtypes by Race/Ethnicity, Poverty, and State
Erratum in
-
Erratum.J Natl Cancer Inst. 2015 Apr 13;107(5):djv121. doi: 10.1093/jnci/djv121. Print 2015 May. J Natl Cancer Inst. 2015. PMID: 25868472 Free PMC article. No abstract available.
-
Erratum.J Natl Cancer Inst. 2015 Jun 4;107(7):djv177. doi: 10.1093/jnci/djv177. Print 2015 Jul. J Natl Cancer Inst. 2015. PMID: 26044857 Free PMC article. No abstract available.
Abstract
Background: The American Cancer Society (ACS), Centers for Disease Control and Prevention (CDC), National Cancer Institute (NCI), and North American Association of Central Cancer Registries (NAACCR) collaborate annually to produce updated, national cancer statistics. This Annual Report includes a focus on breast cancer incidence by subtype using new, national-level data.
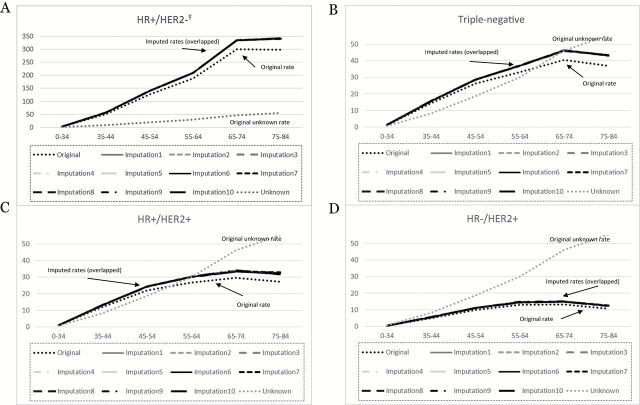
Methods: Population-based cancer trends and breast cancer incidence by molecular subtype were calculated. Breast cancer subtypes were classified using tumor biomarkers for hormone receptor (HR) and human growth factor-neu receptor (HER2) expression.
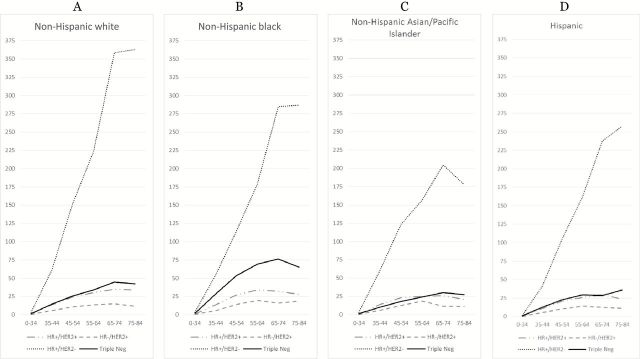
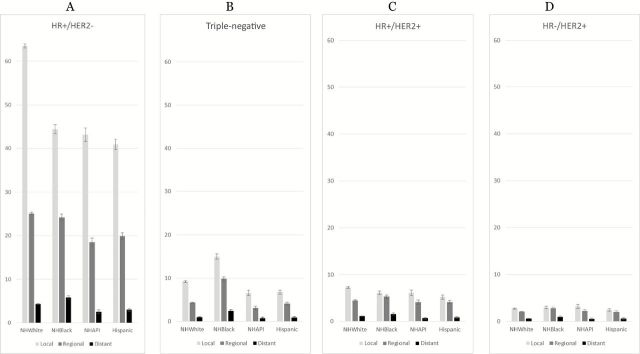
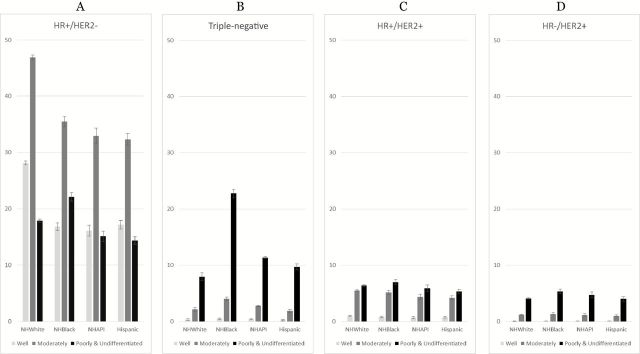
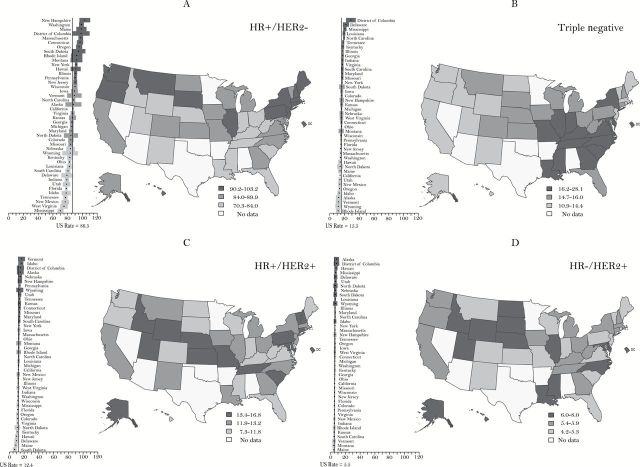
Results: Overall cancer incidence decreased for men by 1.8% annually from 2007 to 2011 [corrected]. Rates for women were stable from 1998 to 2011. Within these trends there was racial/ethnic variation, and some sites have increasing rates. Among children, incidence rates continued to increase by 0.8% per year over the past decade while, like adults, mortality declined. HR+/HER2- breast cancers, the subtype with the best prognosis, were the most common for all races/ethnicities with highest rates among non-Hispanic white women, local stage cases, and low poverty areas (92.7, 63.51, and 98.69 per 100000 non-Hispanic white women, respectively). HR+/HER2- breast cancer incidence rates were strongly, positively correlated with mammography use, particularly for non-Hispanic white women (Pearson 0.57, two-sided P < .001). Triple-negative breast cancers, the subtype with the worst prognosis, were highest among non-Hispanic black women (27.2 per 100000 non-Hispanic black women), which is reflected in high rates in southeastern states.
Conclusions: Progress continues in reducing the burden of cancer in the United States. There are unique racial/ethnic-specific incidence patterns for breast cancer subtypes; likely because of both biologic and social risk factors, including variation in mammography use. Breast cancer subtype analysis confirms the capacity of cancer registries to adjust national collection standards to produce clinically relevant data based on evolving medical knowledge.
© The Author 2015. Published by Oxford University Press.
Figures

Similar articles
-
Age-specific incidence of breast cancer subtypes: understanding the black-white crossover.J Natl Cancer Inst. 2012 Jul 18;104(14):1094-101. doi: 10.1093/jnci/djs264. Epub 2012 Jul 5. J Natl Cancer Inst. 2012. PMID: 22773826 Free PMC article.
-
Variation in Breast Cancer Subtype Incidence and Distribution by Race/Ethnicity in the United States From 2010 to 2015.JAMA Netw Open. 2020 Oct 1;3(10):e2020303. doi: 10.1001/jamanetworkopen.2020.20303. JAMA Netw Open. 2020. PMID: 33074325 Free PMC article.
-
Age/race differences in HER2 testing and in incidence rates for breast cancer triple subtypes: a population-based study and first report.Cancer. 2010 Jun 1;116(11):2549-59. doi: 10.1002/cncr.25016. Cancer. 2010. PMID: 20336785
-
The influence of socioeconomic disparities on breast cancer tumor biology and prognosis: a review.J Womens Health (Larchmt). 2009 Jun;18(6):883-93. doi: 10.1089/jwh.2008.1127. J Womens Health (Larchmt). 2009. PMID: 19514831 Review.
-
Annual report to the nation on the status of cancer, 1975-2000, featuring the uses of surveillance data for cancer prevention and control.J Natl Cancer Inst. 2003 Sep 3;95(17):1276-99. doi: 10.1093/jnci/djg040. J Natl Cancer Inst. 2003. PMID: 12953083 Review.
Cited by
-
Racial disparities in presenting stage and surgical management among octogenarians with breast cancer: a national cancer database analysis.Breast Cancer Res Treat. 2024 Nov 4. doi: 10.1007/s10549-024-07531-3. Online ahead of print. Breast Cancer Res Treat. 2024. PMID: 39495434
-
A microRNA/Runx1/Runx2 network regulates prostate tumor progression from onset to adenocarcinoma in TRAMP mice.Oncotarget. 2016 Oct 25;7(43):70462-70474. doi: 10.18632/oncotarget.11992. Oncotarget. 2016. PMID: 27634876 Free PMC article.
-
Mammography use and breast cancer incidence among older U.S. women.Breast Cancer Res Treat. 2021 Jul;188(1):307-316. doi: 10.1007/s10549-021-06160-4. Epub 2021 Mar 5. Breast Cancer Res Treat. 2021. PMID: 33666831 Free PMC article.
-
Improving early diagnosis of symptomatic cancer.Nat Rev Clin Oncol. 2016 Dec;13(12):740-749. doi: 10.1038/nrclinonc.2016.109. Epub 2016 Jul 26. Nat Rev Clin Oncol. 2016. PMID: 27458007 Review.
-
Demoralization and Its Association with Quality of Life, Sleep Quality, Spiritual Interests, and Suicide Risk in Breast Cancer Inpatients: A Cross-Sectional Study.Int J Environ Res Public Health. 2022 Oct 6;19(19):12815. doi: 10.3390/ijerph191912815. Int J Environ Res Public Health. 2022. PMID: 36232107 Free PMC article.
References
-
- Wingo PA, Ries LA, Rosenberg HM, Miller DS, Edwards BK. Cancer incidence and mortality, 1973–1995: a report card for the U.S. Cancer. 1998;82(6):1197–1207. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
