

BRAF mutation and CDKN2A deletion define a clinically distinct subgroup of childhood secondary high-grade glioma
- PMID: 25667294
- PMCID: PMC4356711
- DOI: 10.1200/JCO.2014.58.3922
BRAF mutation and CDKN2A deletion define a clinically distinct subgroup of childhood secondary high-grade glioma
Abstract
Purpose: To uncover the genetic events leading to transformation of pediatric low-grade glioma (PLGG) to secondary high-grade glioma (sHGG).
Patients and methods: We retrospectively identified patients with sHGG from a population-based cohort of 886 patients with PLGG with long clinical follow-up. Exome sequencing and array CGH were performed on available samples followed by detailed genetic analysis of the entire sHGG cohort. Clinical and outcome data of genetically distinct subgroups were obtained.
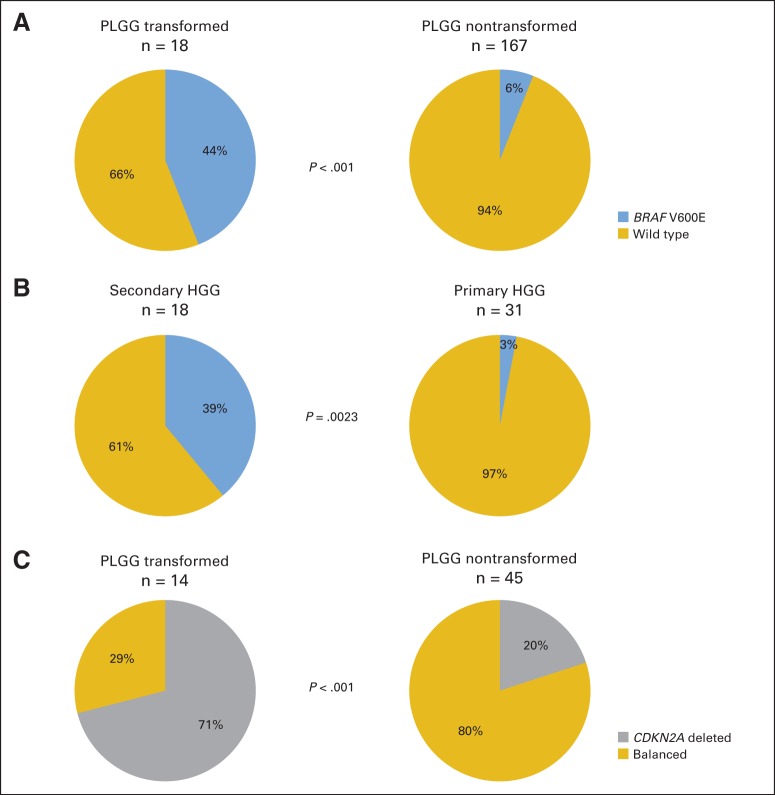
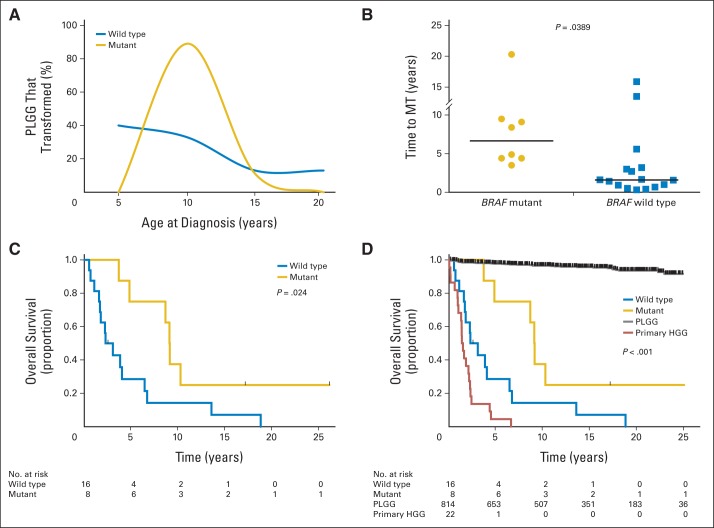
Results: sHGG was observed in 2.9% of PLGGs (26 of 886 patients). Patients with sHGG had a high frequency of nonsilent somatic mutations compared with patients with primary pediatric high-grade glioma (HGG; median, 25 mutations per exome; P = .0042). Alterations in chromatin-modifying genes and telomere-maintenance pathways were commonly observed, whereas no sHGG harbored the BRAF-KIAA1549 fusion. The most recurrent alterations were BRAF V600E and CDKN2A deletion in 39% and 57% of sHGGs, respectively. Importantly, all BRAF V600E and 80% of CDKN2A alterations could be traced back to their PLGG counterparts. BRAF V600E distinguished sHGG from primary HGG (P = .0023), whereas BRAF and CDKN2A alterations were less commonly observed in PLGG that did not transform (P < .001 and P < .001 respectively). PLGGs with BRAF mutations had longer latency to transformation than wild-type PLGG (median, 6.65 years [range, 3.5 to 20.3 years] v 1.59 years [range, 0.32 to 15.9 years], respectively; P = .0389). Furthermore, 5-year overall survival was 75% ± 15% and 29% ± 12% for children with BRAF mutant and wild-type tumors, respectively (P = .024).
Conclusion: BRAF V600E mutations and CDKN2A deletions constitute a clinically distinct subtype of sHGG. The prolonged course to transformation for BRAF V600E PLGGs provides an opportunity for surgical interventions, surveillance, and targeted therapies to mitigate the outcome of sHGG.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures

Comment in
-
Malignant transformation of low-grade gliomas in children: lessons learned from rare medical events.J Clin Oncol. 2015 Mar 20;33(9):978-9. doi: 10.1200/JCO.2014.60.1823. Epub 2015 Feb 9. J Clin Oncol. 2015. PMID: 25667289 No abstract available.
Similar articles
-
Therapeutic and Prognostic Implications of BRAF V600E in Pediatric Low-Grade Gliomas.J Clin Oncol. 2017 Sep 1;35(25):2934-2941. doi: 10.1200/JCO.2016.71.8726. Epub 2017 Jul 20. J Clin Oncol. 2017. PMID: 28727518 Free PMC article.
-
A clinicopathologic study of diencephalic pediatric low-grade gliomas with BRAF V600 mutation.Acta Neuropathol. 2015 Oct;130(4):575-85. doi: 10.1007/s00401-015-1467-3. Epub 2015 Aug 12. Acta Neuropathol. 2015. PMID: 26264609
-
BRAF V600E mutation and 9p21: CDKN2A/B and MTAP co-deletions - Markers in the clinical stratification of pediatric gliomas.BMC Cancer. 2018 Dec 17;18(1):1259. doi: 10.1186/s12885-018-5120-0. BMC Cancer. 2018. PMID: 30558563 Free PMC article.
-
Type II RAF inhibitor tovorafenib for the treatment of pediatric low-grade glioma.Expert Rev Clin Pharmacol. 2024 Nov;17(11):999-1008. doi: 10.1080/17512433.2024.2418405. Epub 2024 Oct 19. Expert Rev Clin Pharmacol. 2024. PMID: 39412085 Review.
-
Paediatric Gliomas: BRAF and Histone H3 as Biomarkers, Therapy and Perspective of Liquid Biopsies.Cancers (Basel). 2021 Feb 4;13(4):607. doi: 10.3390/cancers13040607. Cancers (Basel). 2021. PMID: 33557011 Free PMC article. Review.
Cited by
-
Outcomes of BRAF V600E Pediatric Gliomas Treated With Targeted BRAF Inhibition.JCO Precis Oncol. 2020 May 20;4:PO.19.00298. doi: 10.1200/PO.19.00298. eCollection 2020. JCO Precis Oncol. 2020. PMID: 32923898 Free PMC article.
-
Pan-Cancer and Single-Cell Modeling of Genomic Alterations Through Gene Expression.Front Genet. 2019 Jul 18;10:671. doi: 10.3389/fgene.2019.00671. eCollection 2019. Front Genet. 2019. PMID: 31379928 Free PMC article.
-
Use of bevacizumab as a single agent or in adjunct with traditional chemotherapy regimens in children with unresectable or progressive low-grade glioma.Cancer Med. 2019 Jan;8(1):40-50. doi: 10.1002/cam4.1799. Epub 2018 Dec 19. Cancer Med. 2019. PMID: 30569607 Free PMC article.
-
Long Non-coding RNA and mRNA Co-expression Network Reveals Novel Players in Pleomorphic Xanthoastrocytoma.Mol Neurobiol. 2022 Aug;59(8):5149-5167. doi: 10.1007/s12035-022-02893-5. Epub 2022 Jun 8. Mol Neurobiol. 2022. PMID: 35674862
-
Personalized Treatment of H3K27M-Mutant Pediatric Diffuse Gliomas Provides Improved Therapeutic Opportunities.Front Oncol. 2020 Jan 10;9:1436. doi: 10.3389/fonc.2019.01436. eCollection 2019. Front Oncol. 2020. PMID: 31998633 Free PMC article.
References
-
- Broniscer A, Baker SJ, West AN, et al. Clinical and molecular characteristics of malignant transformation of low-grade glioma in children. J Clin Oncol. 2007;25:682–689. - PubMed
-
- Krieger MD, Gonzalez-Gomez I, Levy ML, et al. Recurrence patterns and anaplastic change in a long-term study of pilocytic astrocytomas. Pediatr Neurosurg. 1997;27:1–11. - PubMed
-
- Dirks PB, Jay V, Becker LE, et al. Development of anaplastic changes in low-grade astrocytomas of childhood. Neurosurgery. 1994;34:68–78. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
