

Comparison of coronary artery calcium presence, carotid plaque presence, and carotid intima-media thickness for cardiovascular disease prediction in the Multi-Ethnic Study of Atherosclerosis
- PMID: 25596139
- PMCID: PMC4299916
- DOI: 10.1161/CIRCIMAGING.114.002262
Comparison of coronary artery calcium presence, carotid plaque presence, and carotid intima-media thickness for cardiovascular disease prediction in the Multi-Ethnic Study of Atherosclerosis
Abstract
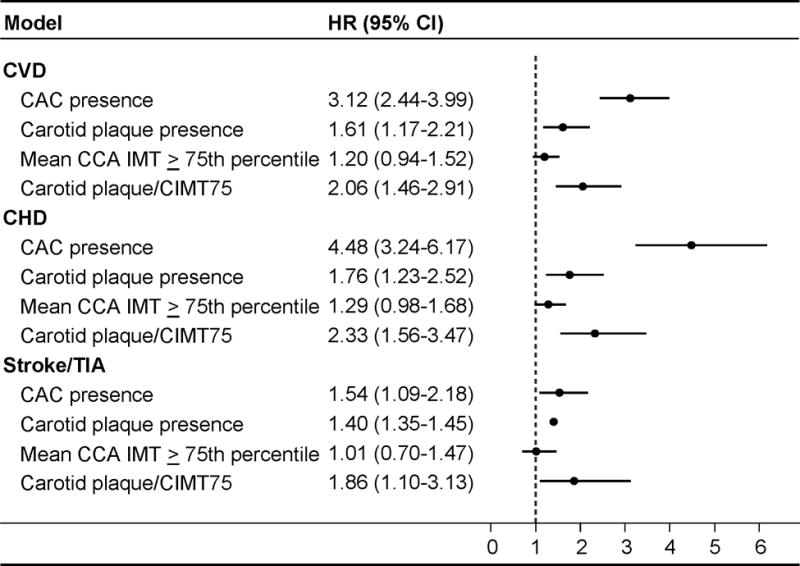
Background: Presence of coronary artery calcium (CAC), carotid plaque, and increased carotid intima-media thickness (IMT) may indicate elevated cardiovascular disease (CVD) risk; however, no large studies have compared them directly. This study compares predictive uses of CAC presence, carotid artery plaque presence, and high IMT for incident CVD events.
Methods and results: Participants were from the Multi-Ethnic Study of Atherosclerosis (MESA). Predictive values of carotid plaque, IMT, and CAC presence were compared using Cox proportional hazards models, c-statistics, and net reclassification indices. The 6779 participants were mean (SD) 62.2 (10.2) years old; 49.9% had CAC, and 46.7% had carotid plaque. The mean left and right IMT were 0.754 (0.210) mm and 0.751 (0.187) mm, respectively. After 9.5 years (mean), 538 CVD events, 388 coronary heart disease (CHD) events, and 196 stroke/transient ischemic attacks were observed. CAC presence was a stronger predictor of incident CVD and CHD than carotid ultrasound measures. Mean IMT≥75th percentile (for age, sex, and race) alone did not predict events. Compared with traditional risk factors, c-statistics for CVD (c=0.756) and CHD (c=0.752) increased the most by the addition of CAC presence (CVD, 0.776; CHD, 0.784; P<0.001) followed by carotid plaque presence (CVD, c=0.760; CHD, c=0.757; P<0.05). Compared with risk factors (c=0.782), carotid plaque presence (c=0.787; P=0.045) but not CAC (c=0.785; P=0.438) improved prediction of stroke/transient ischemic attacks.
Conclusions: In adults without CVD, CAC presence improves prediction of CVD and CHD more than carotid plaque presence or high IMT. CAC and carotid ultrasound parameters performed similarly for stroke/transient ischemic attack event prediction.
Keywords: atherosclerosis; cardiovascular disease; carotid arteries; neuroimaging; risk factors.
© 2015 American Heart Association, Inc.
Figures
Similar articles
-
Comparison of Carotid Plaque Score and Coronary Artery Calcium Score for Predicting Cardiovascular Disease Events: The Multi-Ethnic Study of Atherosclerosis.J Am Heart Assoc. 2017 Feb 14;6(2):e005179. doi: 10.1161/JAHA.116.005179. J Am Heart Assoc. 2017. PMID: 28196817 Free PMC article.
-
Coronary artery calcium and carotid artery intima-media thickness for the prediction of stroke and benefit from statins.Eur J Prev Cardiol. 2018 Dec;25(18):1980-1987. doi: 10.1177/2047487318798058. Epub 2018 Sep 5. Eur J Prev Cardiol. 2018. PMID: 30183342
-
Ischemic stroke/transient ischemic attack events and carotid artery disease in the absence of or with minimal coronary artery calcification: Results from the Multi-Ethnic Study of Atherosclerosis.Atherosclerosis. 2018 Aug;275:22-27. doi: 10.1016/j.atherosclerosis.2018.05.027. Epub 2018 May 17. Atherosclerosis. 2018. PMID: 29852401 Free PMC article.
-
Carotid Intima-Media Thickness as Surrogate for and Predictor of CVD.Glob Heart. 2016 Sep;11(3):295-312.e3. doi: 10.1016/j.gheart.2016.08.006. Glob Heart. 2016. PMID: 27741977 Review.
-
Association of polygenic risk scores with incident atherosclerotic cardiovascular disease events among individuals with coronary artery calcium score of zero: The multi-ethnic study of atherosclerosis.Prog Cardiovasc Dis. 2022 Sep-Oct;74:19-27. doi: 10.1016/j.pcad.2022.08.003. Epub 2022 Aug 8. Prog Cardiovasc Dis. 2022. PMID: 35952728 Free PMC article. Review.
Cited by
-
Association of Carotid Artery Plaque With Cardiovascular Events and Incident Coronary Artery Calcium in Individuals With Absent Coronary Calcification: The MESA.Circ Cardiovasc Imaging. 2021 Apr;14(4):e011701. doi: 10.1161/CIRCIMAGING.120.011701. Epub 2021 Apr 8. Circ Cardiovasc Imaging. 2021. PMID: 33827231 Free PMC article.
-
Cholesterol Mass Efflux Capacity, Incident Cardiovascular Disease, and Progression of Carotid Plaque.Arterioscler Thromb Vasc Biol. 2019 Jan;39(1):89-96. doi: 10.1161/ATVBAHA.118.311366. Arterioscler Thromb Vasc Biol. 2019. PMID: 30580560 Free PMC article.
-
Vascular Cognitive Impairment (VCI).Neurotherapeutics. 2022 Jan;19(1):68-88. doi: 10.1007/s13311-021-01170-y. Epub 2021 Dec 22. Neurotherapeutics. 2022. PMID: 34939171 Free PMC article. Review.
-
Coronary Calcium Characteristics as Predictors of Major Adverse Cardiac Events in Symptomatic Patients: Insights From the CORE 320 Multinational Study.J Am Heart Assoc. 2019 Mar 19;8(6):e007201. doi: 10.1161/JAHA.117.007201. J Am Heart Assoc. 2019. PMID: 30879377 Free PMC article.
-
Association of traditional risk factors with carotid intima-media thickness and carotid plaque in asymptomatic individuals with a family history of premature cardiovascular disease.Int J Cardiovasc Imaging. 2022 Apr;38(4):739-749. doi: 10.1007/s10554-021-02459-x. Epub 2021 Nov 3. Int J Cardiovasc Imaging. 2022. PMID: 34731395
References
-
- Folsom AR, Kronmal RA, Detrano RC, O’Leary DH, Bild DE, Bluemke DA, Budoff MJ, Liu K, Shea S, Szklo M, Tracy RP, Watson KE, Burke GL. Coronary artery calcification compared with carotid intima-media thickness in the prediction of cardiovascular disease incidence: the Multi-Ethnic Study of Atherosclerosis (MESA) Arch Intern Med. 2008;168:1333–1339. - PMC - PubMed
-
- Greenland P, Bonow RO, Brundage BH, Budoff MJ, Eisenberg MJ, Grundy SM, Lauer MS, Post WS, Raggi P, Redberg RF, Rodgers GP, Shaw LJ, Taylor AJ, Weintraub WS, Harrington RA, Abrams J, Anderson JL, Bates ER, Grines CL, Hlatky MA, Lichtenberg RC, Lindner JR, Pohost GM, Schofield RS, Shubrooks SJ, Jr, Stein JH, Tracy CM, Vogel RA, Wesley DJ. ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) Circulation. 2007;115:402–426. - PubMed
-
- Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, Najjar SS, Rembold CM, Post WS. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr. 2008;21:93–111. - PubMed
Publication types
MeSH terms
Grants and funding
- T32 HL007936/HL/NHLBI NIH HHS/United States
- N01-HC-95162/HC/NHLBI NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- UL1-RR-025005/RR/NCRR NIH HHS/United States
- N01 HC095167/HC/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01-HC-95163/HC/NHLBI NIH HHS/United States
- N01-HC-95168/HC/NHLBI NIH HHS/United States
- N01HC95169/HL/NHLBI NIH HHS/United States
- UL1-RR-024156/RR/NCRR NIH HHS/United States
- N01 HC095161/HC/NHLBI NIH HHS/United States
- UL1 RR024156/RR/NCRR NIH HHS/United States
- N01 HC095164/HC/NHLBI NIH HHS/United States
- N01-HC-95159/HC/NHLBI NIH HHS/United States
- N01 HC095166/HC/NHLBI NIH HHS/United States
- N01-HC-95165/HC/NHLBI NIH HHS/United States
- N01 HC095160/HC/NHLBI NIH HHS/United States
- T32 HL 07936/HL/NHLBI NIH HHS/United States
- P50 ES015915/ES/NIEHS NIH HHS/United States
- N01-HC-95169/HC/NHLBI NIH HHS/United States
- N01-HC-95164/HC/NHLBI NIH HHS/United States
- N01HC95159/HL/NHLBI NIH HHS/United States
- N01 HC095169/HC/NHLBI NIH HHS/United States
- N01-HC-95160/HC/NHLBI NIH HHS/United States
- N01 HC095165/HC/NHLBI NIH HHS/United States
- N01 HC095168/HC/NHLBI NIH HHS/United States
- N01-HC-95161/HC/NHLBI NIH HHS/United States
- ES015915/ES/NIEHS NIH HHS/United States
- N01 HC095163/HC/NHLBI NIH HHS/United States
- N01-HC-95166/HC/NHLBI NIH HHS/United States
- N01 HC095162/HC/NHLBI NIH HHS/United States
- N01 HC095159/HC/NHLBI NIH HHS/United States
- N01-HC-95167/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
