

Genetically low vitamin D concentrations and increased mortality: Mendelian randomisation analysis in three large cohorts
- PMID: 25406188
- PMCID: PMC4238742
- DOI: 10.1136/bmj.g6330
Genetically low vitamin D concentrations and increased mortality: Mendelian randomisation analysis in three large cohorts
Abstract
Objective: To test the hypothesis that genetically low 25-hydroxyvitamin D concentrations are associated with increased mortality.
Design: Mendelian randomisation analysis.
Setting: Copenhagen City Heart Study, Copenhagen General Population Study, and Copenhagen Ischemic Heart Disease Study.
Participants: 95 766 white participants of Danish descent from three cohorts, with median follow-up times of 19.1, 5.8, and 7.9 years, genotyped for genetic variants in DHCR7 and CYP2R1 affecting plasma 25-hydroxyvitamin D concentrations; 35 334 also had plasma 25-hydroxyvitamin D measurements. Participants were followed from study entry through 2013, during which time 10 349 died.
Main outcome measures: All cause mortality and cause specific mortality, adjusted for common risk factors for all cause mortality based on the World Health Organization's global health status.
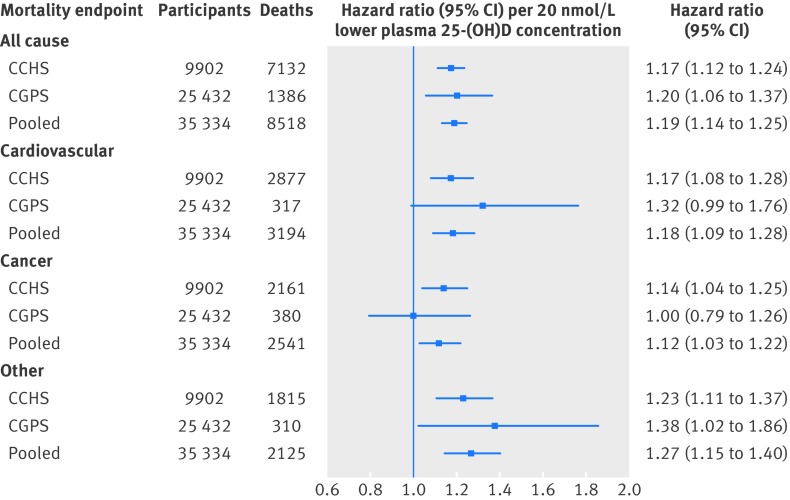
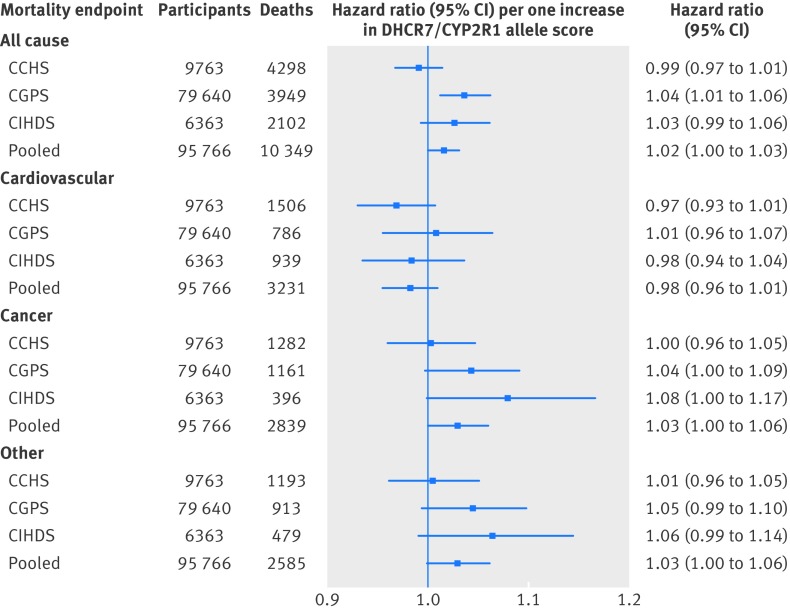
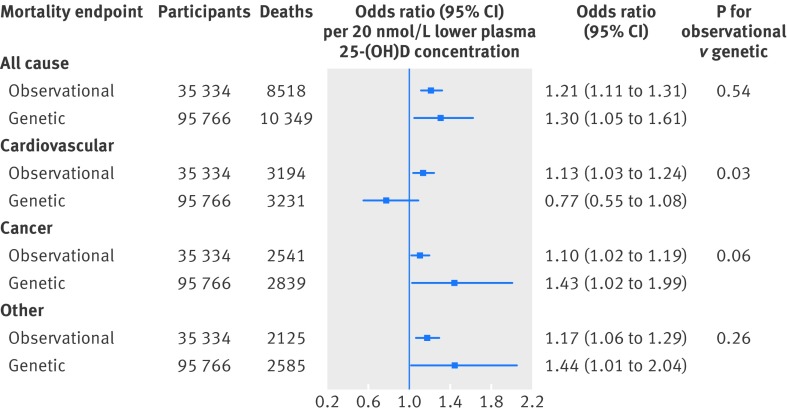
Results: The multivariable adjusted hazard ratios for a 20 nmol/L lower plasma 25-hydroxyvitamin D concentration were 1.19 (95% confidence interval 1.14 to 1.25) for all cause mortality, 1.18 (1.09 to 1.28) for cardiovascular mortality, 1.12 (1.03 to 1.22) for cancer mortality, and 1.27 (1.15 to 1.40) for other mortality. Each increase in DHCR7/CYP2R1 allele score was associated with a 1.9 nmol/L lower plasma 25-hydroxyvitamin D concentration and with increased all cause, cancer, and other mortality but not with cardiovascular mortality. The odds ratio for a genetically determined 20 nmol/L lower plasma 25-hydroxyvitamin D concentration was 1.30 (1.05 to 1.61) for all cause mortality, with a corresponding observational multivariable adjusted odds ratio of 1.21 (1.11 to 1.31). Corresponding genetic and observational odds ratios were 0.77 (0.55 to 1.08) and 1.13 (1.03 to 1.24) for cardiovascular mortality, 1.43 (1.02 to 1.99) and 1.10 (1.02 to 1.19) for cancer mortality, and 1.44 (1.01 to 2.04) and 1.17 (1.06 to 1.29) for other mortality. The results were robust in sensitivity analyses.
Conclusions: Genetically low 25-hydroxyvitamin D concentrations were associated with increased all cause mortality, cancer mortality, and other mortality but not with increased cardiovascular mortality. These findings are compatible with the notion that genetically low 25-hydroxyvitamin D concentrations may be causally associated with cancer and other mortality but also suggest that the observational association with cardiovascular mortality could be the result of confounding.
© Afzal et al 2014.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures

Comment in
-
Vitamin D genes and mortality.BMJ. 2014 Nov 18;349:g6599. doi: 10.1136/bmj.g6599. BMJ. 2014. PMID: 25406190 No abstract available.
Similar articles
-
No evidence that genetically reduced 25-hydroxyvitamin D is associated with increased risk of ischaemic heart disease or myocardial infarction: a Mendelian randomization study.Int J Epidemiol. 2015 Apr;44(2):651-61. doi: 10.1093/ije/dyv078. Epub 2015 May 16. Int J Epidemiol. 2015. PMID: 25981321
-
Low vitamin D and risk of bacterial pneumonias: Mendelian randomisation studies in two population-based cohorts.Thorax. 2021 May;76(5):468-478. doi: 10.1136/thoraxjnl-2020-215288. Epub 2020 Oct 27. Thorax. 2021. PMID: 33109689
-
Vitamin D and Inflammatory Bowel Disease: Mendelian Randomization Analyses in the Copenhagen Studies and UK Biobank.J Clin Endocrinol Metab. 2018 Sep 1;103(9):3267-3277. doi: 10.1210/jc.2018-00250. J Clin Endocrinol Metab. 2018. PMID: 29947775
-
The relationship of vitamin D status to risk of cardiovascular disease and mortality.Dan Med J. 2015 Feb;62(2):B5008. Dan Med J. 2015. PMID: 25634511 Review.
-
Vitamin D concentration, obesity, and risk of diabetes: a mendelian randomisation study.Lancet Diabetes Endocrinol. 2014 Apr;2(4):298-306. doi: 10.1016/S2213-8587(13)70200-6. Epub 2014 Jan 28. Lancet Diabetes Endocrinol. 2014. PMID: 24703048 Review.
Cited by
-
Applying Mendelian randomization to appraise causality in relationships between nutrition and cancer.Cancer Causes Control. 2022 May;33(5):631-652. doi: 10.1007/s10552-022-01562-1. Epub 2022 Mar 11. Cancer Causes Control. 2022. PMID: 35274198 Free PMC article.
-
Association between Blood 25-Hydroxyvitamin D Levels and Survival in Colorectal Cancer Patients: An Updated Systematic Review and Meta-Analysis.Nutrients. 2018 Jul 13;10(7):896. doi: 10.3390/nu10070896. Nutrients. 2018. PMID: 30011816 Free PMC article. Review.
-
Vitamin D testing and treatment: a narrative review of current evidence.Endocr Connect. 2019 Feb 1;8(2):R27-R43. doi: 10.1530/EC-18-0432. Endocr Connect. 2019. PMID: 30650061 Free PMC article. Review.
-
Circulating 25-hydroxyvitamin D up to 3 decades prior to diagnosis in relation to overall and organ-specific cancer survival.Eur J Epidemiol. 2018 Nov;33(11):1087-1099. doi: 10.1007/s10654-018-0428-2. Epub 2018 Aug 2. Eur J Epidemiol. 2018. PMID: 30073448 Free PMC article.
-
Vitamin-D Deficiency and Supplementation Altered the Network of the Coronary Arteries in a Rodent Model-In Situ Video Microscopic Technique.Nutrients. 2022 May 13;14(10):2041. doi: 10.3390/nu14102041. Nutrients. 2022. PMID: 35631182 Free PMC article.
References
-
- Smith GD, Ebrahim S. Mendelian randomization: prospects, potentials, and limitations. Int J Epidemiol 2004;33:30-42. - PubMed
-
- Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey SG. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med 2008;27:1133-63. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous