

HDL cholesterol efflux capacity and incident cardiovascular events
- PMID: 25404125
- PMCID: PMC4308988
- DOI: 10.1056/NEJMoa1409065
HDL cholesterol efflux capacity and incident cardiovascular events
Abstract
Background: It is unclear whether high-density lipoprotein (HDL) cholesterol concentration plays a causal role in atherosclerosis. A more important factor may be HDL cholesterol efflux capacity, the ability of HDL to accept cholesterol from macrophages, which is a key step in reverse cholesterol transport. We investigated the epidemiology of cholesterol efflux capacity and its association with incident atherosclerotic cardiovascular disease outcomes in a large, multiethnic population cohort.
Methods: We measured HDL cholesterol level, HDL particle concentration, and cholesterol efflux capacity at baseline in 2924 adults free from cardiovascular disease who were participants in the Dallas Heart Study, a probability-based population sample. The primary end point was atherosclerotic cardiovascular disease, defined as a first nonfatal myocardial infarction, nonfatal stroke, or coronary revascularization or death from cardiovascular causes. The median follow-up period was 9.4 years.
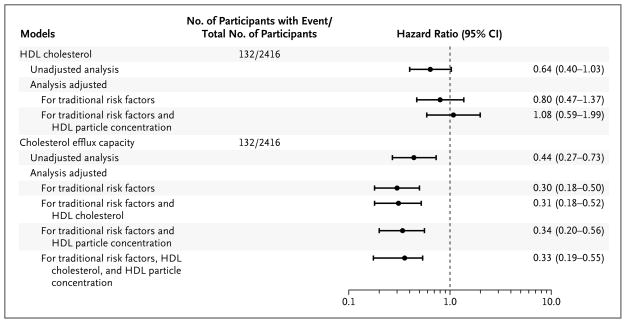
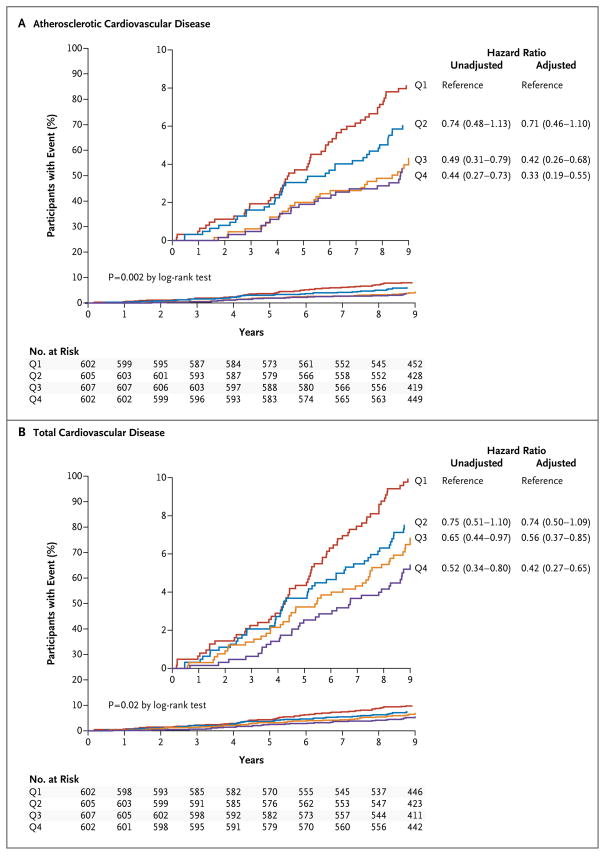
Results: In contrast to HDL cholesterol level, which was associated with multiple traditional risk factors and metabolic variables, cholesterol efflux capacity had minimal association with these factors. Baseline HDL cholesterol level was not associated with cardiovascular events in an adjusted analysis (hazard ratio, 1.08; 95% confidence interval [CI], 0.59 to 1.99). In a fully adjusted model that included traditional risk factors, HDL cholesterol level, and HDL particle concentration, there was a 67% reduction in cardiovascular risk in the highest quartile of cholesterol efflux capacity versus the lowest quartile (hazard ratio, 0.33; 95% CI, 0.19 to 0.55). Adding cholesterol efflux capacity to traditional risk factors was associated with improvement in discrimination and reclassification indexes.
Conclusions: Cholesterol efflux capacity, a new biomarker that characterizes a key step in reverse cholesterol transport, was inversely associated with the incidence of cardiovascular events in a population-based cohort. (Funded by the Donald W. Reynolds Foundation and others.).
Figures
Comment in
-
Atherosclerosis: cholesterol efflux capacity-a new biomarker for cardiovascular risk?Nat Rev Cardiol. 2015 Jan;12(1):2. doi: 10.1038/nrcardio.2014.198. Epub 2014 Dec 2. Nat Rev Cardiol. 2015. PMID: 25445136 No abstract available.
-
Biomarkers: Cholesterol efflux capacity--inverse association with incident cardiovascular disease.Nat Rev Endocrinol. 2015 Feb;11(2):64. doi: 10.1038/nrendo.2014.217. Epub 2014 Dec 9. Nat Rev Endocrinol. 2015. PMID: 25488484 No abstract available.
-
HDL cholesterol efflux capacity and cardiovascular events.N Engl J Med. 2015 May 7;372(19):1871-2. doi: 10.1056/NEJMc1503139. N Engl J Med. 2015. PMID: 25946297 No abstract available.
-
HDL cholesterol efflux capacity and cardiovascular events.N Engl J Med. 2015 May 7;372(19):1869. doi: 10.1056/NEJMc1503139. N Engl J Med. 2015. PMID: 25946298 No abstract available.
-
HDL cholesterol efflux capacity and cardiovascular events.N Engl J Med. 2015 May 7;372(19):1869. doi: 10.1056/NEJMc1503139. N Engl J Med. 2015. PMID: 25946299 No abstract available.
-
HDL cholesterol efflux capacity and cardiovascular events.N Engl J Med. 2015 May 7;372(19):1870-1. doi: 10.1056/NEJMc1503139. N Engl J Med. 2015. PMID: 25946300 No abstract available.
-
HDL cholesterol efflux capacity and cardiovascular events.N Engl J Med. 2015 May 7;372(19):1871. doi: 10.1056/NEJMc1503139. N Engl J Med. 2015. PMID: 25946301 No abstract available.
-
Cholesterol efflux capacity as a novel biomarker for incident cardiovascular events: has high-density lipoprotein been resuscitated?Circ Res. 2015 May 8;116(10):1646-8. doi: 10.1161/CIRCRESAHA.115.305938. Circ Res. 2015. PMID: 25953923 No abstract available.
Similar articles
-
Cholesterol Efflux Capacity, High-Density Lipoprotein Particle Number, and Incident Cardiovascular Events: An Analysis From the JUPITER Trial (Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin).Circulation. 2017 Jun 20;135(25):2494-2504. doi: 10.1161/CIRCULATIONAHA.116.025678. Epub 2017 Apr 27. Circulation. 2017. PMID: 28450350 Free PMC article. Clinical Trial.
-
Association of the serum myeloperoxidase/high-density lipoprotein particle ratio and incident cardiovascular events in a multi-ethnic population: Observations from the Dallas Heart Study.Atherosclerosis. 2017 Aug;263:156-162. doi: 10.1016/j.atherosclerosis.2017.06.007. Epub 2017 Jun 3. Atherosclerosis. 2017. PMID: 28645072 Free PMC article.
-
High-density lipoprotein cholesterol efflux capacity is inversely associated with cardiovascular risk: a systematic review and meta-analysis.Lipids Health Dis. 2017 Nov 10;16(1):212. doi: 10.1186/s12944-017-0604-5. Lipids Health Dis. 2017. PMID: 29126414 Free PMC article. Review.
-
Cholesterol efflux capacity is an independent predictor of all-cause and cardiovascular mortality in patients with coronary artery disease: A prospective cohort study.Atherosclerosis. 2016 Jun;249:116-24. doi: 10.1016/j.atherosclerosis.2015.10.111. Epub 2015 Nov 10. Atherosclerosis. 2016. PMID: 27088866
-
HDL Cholesterol Efflux Capacity: Cardiovascular Risk Factor and Potential Therapeutic Target.Curr Atheroscler Rep. 2016 Jan;18(1):2. doi: 10.1007/s11883-015-0554-1. Curr Atheroscler Rep. 2016. PMID: 26710794 Review.
Cited by
-
Macrophage Mitochondrial Energy Status Regulates Cholesterol Efflux and Is Enhanced by Anti-miR33 in Atherosclerosis.Circ Res. 2015 Jul 17;117(3):266-78. doi: 10.1161/CIRCRESAHA.117.305624. Epub 2015 May 22. Circ Res. 2015. PMID: 26002865 Free PMC article.
-
Systemic consequences of abnormal cholesterol handling: Interdependent pathways of inflammation and dyslipidemia.Front Immunol. 2022 Aug 26;13:972140. doi: 10.3389/fimmu.2022.972140. eCollection 2022. Front Immunol. 2022. PMID: 36091062 Free PMC article. Review.
-
Beyond Coronary Calcification, Family History, and C-Reactive Protein: Cholesterol Efflux Capacity and Cardiovascular Risk Prediction.J Am Coll Cardiol. 2016 May 31;67(21):2480-7. doi: 10.1016/j.jacc.2016.03.538. J Am Coll Cardiol. 2016. PMID: 27230043 Free PMC article.
-
Variants with large effects on blood lipids and the role of cholesterol and triglycerides in coronary disease.Nat Genet. 2016 Jun;48(6):634-9. doi: 10.1038/ng.3561. Epub 2016 May 2. Nat Genet. 2016. PMID: 27135400 Free PMC article.
-
Effect of open-label infusion of an apoA-I-containing particle (CER-001) on RCT and artery wall thickness in patients with FHA.J Lipid Res. 2015 Mar;56(3):703-712. doi: 10.1194/jlr.M055665. Epub 2015 Jan 5. J Lipid Res. 2015. PMID: 25561459 Free PMC article. Clinical Trial.
References
-
- Stone NJ, Robinson J, Lichtenstein AH, et al. ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(Suppl 2):S1–S45. Erratum, Circulation 2014;129:Suppl 2:S46–S48. - PubMed
-
- Boden WE, Probstfield JL, Anderson T, et al. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med. 2011;365:2255–67. Erratum, N Engl J Med 2012;367:189. - PubMed
-
- Barter PJ, Caulfield M, Eriksson M, et al. Effects of torcetrapib in patients at high risk for coronary events. N Engl J Med. 2007;357:2109–22. - PubMed
-
- Schwartz GG, Olsson AG, Abt M, et al. Effects of dalcetrapib in patients with a recent acute coronary syndrome. N Engl J Med. 2012;367:2089–99. - PubMed
-
- The HPS2-THRIVE Collaborative Group. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med. 2014;371:203–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources