

Gastrointestinal dysfunction in liver cirrhosis
- PMID: 25356031
- PMCID: PMC4209534
- DOI: 10.3748/wjg.v20.i40.14686
Gastrointestinal dysfunction in liver cirrhosis
Abstract
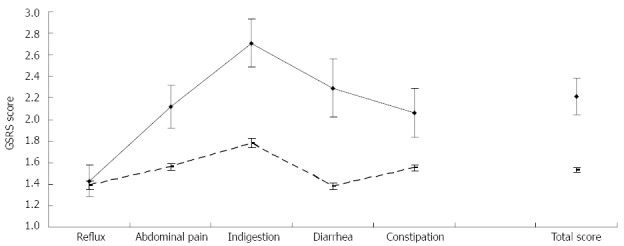
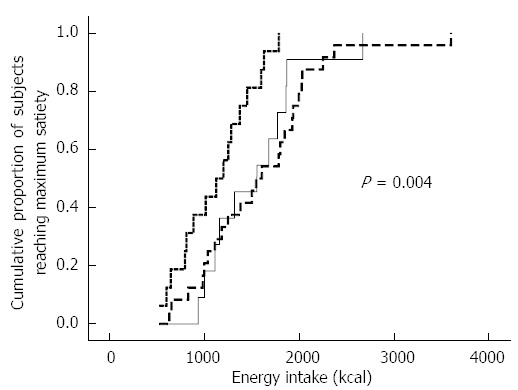
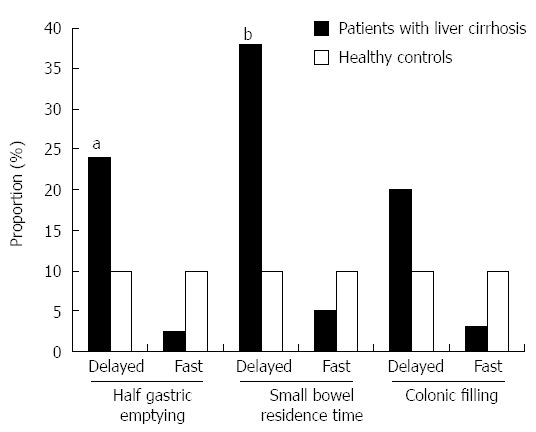
Patients with liver cirrhosis exhibit several features of gut dysfunction which may contribute to the development of cirrhosis complications as well as have an impact on nutritional status and health-related quality of life. Gastrointestinal symptoms are common in cirrhosis and their pathophysiology probably involves factors related to liver disease severity, psychological distress, and gut dysfunction (e.g., increased gastric sensitivity to distension and delayed gut transit). They may lead to reduced food intake and, thus, may contribute to the nutritional status deterioration in cirrhotic patients. Although tense ascites appears to have a negative impact on meal-induced accommodation of the stomach, published data on gastric accommodation in cirrhotics without significant ascites are not unanimous. Gastric emptying and small bowel transit have generally been shown to be prolonged. This may be related to disturbances in postprandial glucose, insulin, and ghrelin levels, which, in turn, appear to be associated to insulin resistance, a common finding in cirrhosis. Furthermore, small bowel manometry disturbances and delayed gut transit may be associated with the development of small bowel bacterial overgrowth. Finally, several studies have reported intestinal barrier dysfunction in patients with cirrhosis (especially those with portal hypertension), which is related to bacterial translocation and permeation of intestinal bacterial products, e.g., endotoxin and bacterial DNA, thus potentially being involved in the pathogenesis of complications of liver cirrhosis.
Keywords: Gastric accommodation; Gastrointestinal symptoms; Gut motility; Intestinal permeability; Liver cirrhosis; Malnutrition.
Figures
Similar articles
-
Gut transit is associated with gastrointestinal symptoms and gut hormone profile in patients with cirrhosis.Clin Gastroenterol Hepatol. 2009 Mar;7(3):346-52. doi: 10.1016/j.cgh.2008.11.022. Epub 2008 Dec 3. Clin Gastroenterol Hepatol. 2009. PMID: 19200458
-
Decompensated cirrhotics have slower intestinal transit times as compared with compensated cirrhotics and healthy controls.J Clin Gastroenterol. 2013 Nov-Dec;47(10):888-93. doi: 10.1097/MCG.0b013e31829006bb. J Clin Gastroenterol. 2013. PMID: 23632359
-
Role of gastric sensorimotor dysfunction in gastrointestinal symptoms and energy intake in liver cirrhosis.Scand J Gastroenterol. 2007 Feb;42(2):237-46. doi: 10.1080/00365520600880898. Scand J Gastroenterol. 2007. PMID: 17327944
-
The pathogenesis of gastrointestinal bacterial overgrowth.Chemotherapy. 2005;51 Suppl 1:1-22. doi: 10.1159/000081988. Chemotherapy. 2005. PMID: 15855746 Review.
-
Gastrointestinal Physiology and Function.Handb Exp Pharmacol. 2017;239:1-16. doi: 10.1007/164_2016_118. Handb Exp Pharmacol. 2017. PMID: 28176047 Review.
Cited by
-
Nutrition in Chronic Liver Disease: Consensus Statement of the Indian National Association for Study of the Liver.J Clin Exp Hepatol. 2021 Jan-Feb;11(1):97-143. doi: 10.1016/j.jceh.2020.09.003. Epub 2020 Oct 1. J Clin Exp Hepatol. 2021. PMID: 33679050 Free PMC article. Review.
-
Metabolomics Research Reveals the Mechanism of Action of Astragalus Polysaccharide in Rats with Digestive System Disorders.Molecules. 2018 Dec 15;23(12):3333. doi: 10.3390/molecules23123333. Molecules. 2018. PMID: 30558291 Free PMC article.
-
STORE-gastrointestinal functions and gastrointestinal hormones in patients with liver failure.Medicine (Baltimore). 2018 Nov;97(48):e13167. doi: 10.1097/MD.0000000000013167. Medicine (Baltimore). 2018. PMID: 30508896 Free PMC article.
-
Prevalence, Recognition, and Risk Factors of Constipation among Medically Hospitalized Patients: A Cohort Prospective Study.Medicina (Kaunas). 2023 Jul 23;59(7):1347. doi: 10.3390/medicina59071347. Medicina (Kaunas). 2023. PMID: 37512158 Free PMC article.
-
Increased Intestinal Permeability and Decreased Barrier Function: Does It Really Influence the Risk of Inflammation?Inflamm Intest Dis. 2016 Oct;1(3):135-145. doi: 10.1159/000447252. Epub 2016 Jul 20. Inflamm Intest Dis. 2016. PMID: 29922669 Free PMC article. Review.
References
-
- Pozzi M, Carugo S, Boari G, Pecci V, de Ceglia S, Maggiolini S, Bolla GB, Roffi L, Failla M, Grassi G, et al. Evidence of functional and structural cardiac abnormalities in cirrhotic patients with and without ascites. Hepatology. 1997;26:1131–1137. - PubMed
-
- Liu H, Song D, Lee SS. Cirrhotic cardiomyopathy. Gastroenterol Clin Biol. 2002;26:842–847. - PubMed
-
- Hoeper MM, Krowka MJ, Strassburg CP. Portopulmonary hypertension and hepatopulmonary syndrome. Lancet. 2004;363:1461–1468. - PubMed
-
- Cárdenas A. Hepatorenal syndrome: a dreaded complication of end-stage liver disease. Am J Gastroenterol. 2005;100:460–467. - PubMed
-
- Pham PT, Pham PC, Rastogi A, Wilkinson AH. Review article: current management of renal dysfunction in the cirrhotic patient. Aliment Pharmacol Ther. 2005;21:949–961. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
